

Ex-vivo study of hybrid energy technology using
a human skin model
Background: More aging adults and the social acceptance of aesthetic treatments have increased the demand for minimally invasive aesthetic treatments. Skin resurfacing is very effective at improving aging symp-toms, including wrinkles and skin imperfections. Following the negative effects of full skin resurfacing, in addition to a very long downtime, fractional lasers and fractional radiofrequency (RF) technologies were introduced, since gaining popularity. Their efficacy, along with minimal downtime, has enabled an effective and safer treatment. A novel tech-nology based on fractional Hybrid EnergyTM (HE), combines RF and an additional electrical energy for enhancing the thermal effect. Objec-tive: This study evaluated the morphological and histological effects of the new HE technology on epidermal and dermal skin layers, using an ex-vivo human skin model. Methods: Human skin samples were collected and treated ex-vivo with the HE applicator. The effect was evaluated by skin histology and quantitative analysis by assays of col-lagen fibers, elastin and glycosaminoglycan (GAGs) dosages, reflecting the hyaluronic acid content, in addition to epidermal mitotic index eval-uation. Results: Histology demonstrated immediate and long-term HE effects on both epidermal and dermal skin layers with a direct correla-tion between the treatment parameters and effects. Results demonstrated a significant increase of the epidermal mitotic index, significant der-mal collagen remodeling and significant increases in both epidermal and dermal GAGs. Conclusions: HE technology significantly affected collagen remodeling and an increase in mid to deep dermis GAGs in addition to epidermal mitotic index, resulting in long term structural and biochemical dermal and epidermal improvement.
Key words: Hybrid Energy, Fractional Radiofrequency, Hyaluronic Acid, Collagen, Ex-Vivo Histology
See also: Geneo Face Rejuvenation Device, Geneo Personal Oxygen Facial at Home
Combinations of factors induce the aging processes of skin; these include intrinsic factors such as changes in hormone levels, particularly estrogen,as well as a decline in metabolic activity and cell regen-eration. Extrinsic factors affecting skin aging include UV exposure (which is the primary extrinsic factor), environ-mental pollution and smoking [1].
As a result, alterations to the skin affect the structure and cellular turnover rate of both the dermis and epidermis, resulting in altered epidermal unity and thinning of the dermis. Collagen fragmenta-tion is a major cause of dermal degradation, affecting not only the quality of existing collagen, but also negatively affecting fibroblast activity [2]. Reduction in fibroblast activity further degrades skin quality through decreased production of new collagen, elastin and GAG (whose main component is hyaluronic acid). These alterations result in increased skin laxity, the appearance of wrinkles and fine lines and a general decline in skin texture and quality.
Skin resurfacing has been established as an effective treatment for a full range of skin aging symptoms and imperfections. Chemical peels and, later, ablative laser skin resurfacing technologies have demonstrated impressive results for the treatment of wrinkles, lax skin, acne scars, dyschromia and for general skin enhancement. Carbon dioxide (CO2) lasers and erbium: yttrium-aluminum-garnet (Erbium YAG) lasers, were first introduced in the mid-1990s, and were considered the gold standard of minimally invasive treatments, due to their efficacy [3-5]. However the significant downtime and the wide range of adverse effects associated with these treatments, especially in Asian and darker skin, created a need for new technologies delivering visible clinical improvement with reduced downtime and lower risk [6].
A fractional treatment method delivers energy to specific small “islets” of tissue, leaving intact skin in-between these treated islets. Healing is initiated from these intact skin areas resulting in reduced downtime and reduced complica-tions with impressive results. Fractional technologies first emerged around 2003 (Reliant) and soon gained popular-ity, leading to the development of a variety of ablative and non-ablative fractional laser options [7, 8].
The introduction of fractional treatment methods opened a window of opportunity for a large population seeking anti-aging aesthetic treatments but not wanting the risk and downtime associated with more aggressive methods. Fractional Radio Frequency (RF) technologies have become an accepted treatment method for skin aging and imperfections and are gaining popularity with physicians in the aesthetic market due their efficacy, safety and mini-mal downtime [9,10]. Fractional RF deploys a matrix of pin electrodes that are placed on the skin surface. The emission of RF energy through the pin electrodes results in areas of epidermal ablation directly under each electrode, accompa-nied with volumetric heating affecting the dermal layer. Recently, devices using fractional RF micro-needle tech-nology have been introduced for the treatment of facial wrinkles, skin tightening and for correction of skin imper-fections such as acne scars and stretch marks [11]. The unique method of administering the treatment energy directly into the dermis via the micro-needles enables a controlled, focused treatment, while minimizing the ther-mal effect on the epidermis, enabling minimal downtime and adverse effects.
Mulholland et al. evaluated the effect of a Fractional abla-tive RF micro-needle technology for skin rejuvenation (FractoraTM by Invasix Ltd.) [12]. Histological findings demonstrated deep ablation and collagen restructuring in the papillary and reticular dermis. The authors concluded that the reduction of wrinkles and the skin tightening achieved was similar to the results seen with fractional ablative CO2 lasers combined with additional non-ablative dermal RF stimulation. In all cases re-epithelialization occurred within4-7days and with no significant adverse effects such as hypo-pigmentation, PIH or hyper-trophic/hypotrophic scars. The authors concluded that the Fractional RF multi-needle technology was effective and safe with less risk of hyper- or hypo-pigmentation on Asian skin, as a result of the direct energy delivery method enabled through micro needles.
The new Hybrid Energy (HE) technology combines dual energy; first, RF energy is applied, which provides a safe and effective penetration and controlled heating of the skin. RF energy is followed by an electrical energy directly applied to the target area to enhance the total clinical effect. The HE energy is delivered in a precisely controlled frac-tional manner via an array of sophisticated micro-needles through the epidermis, up to the mid dermis.
This ex-vivo study was designed to investigate the effects of the HE technology via evaluation and analysis of histolog-ical, morphological and other biometric changes following a HE treatment using the HE applicator on ex-vivo human skin samples.
Materials and methods
Ex-vivo survival model
Skin fragments harvested from 6 donors undergoing face lifts were cut into 3 cm2 sections and washed three times with an antibiotic solution (300 U/mL penicillin and 300 g/mL streptomycin for the first washing procedure). Skin biopsies were placed with the epithelium uppermost, at an air/liquid interface, on culture inserts (filter pore size 12 m) [13]. These inserts were set on 6 well plates and culture medium was added underneath three times a week. The medium used was Dulbecco’s Minimal Essen-tial Medium (DMEM) containing antibiotics (100 U/mL penicillin and 100 g/ml streptomycin), 200 g/mL L-glutamine and growth factors (bovine pituitary extract and fetal calf serum). All supplements were freshly made at each medium change, every two days. Skin biopsies were then put in a humidified atmosphere of 95% air-5% CO2 at 37 ◦C. By using this method the device could be applied directly to the epidermis.
The aging model
The aging model was created using radiation on day 0 and day 1 (D0, D1) with UVA (8 J/cm2) and UV B (2 J/cm2), artificially damaging the skin samples so that they were similar to one another [14]. A Vilber Lourmat simulator (Vilber Lourmat, Marnes-la-Vallée, France) was used to create the ultraviolet irradiation and was fitted out with a UVA radiation source (365 nm) composed of Vilber Lour-mat T-20.L-365 mercury vapor tubes, low pressure and hot cathodes with a Vilber Lourmat RMX-365/312 radiome-ter. The UVB radiation source (312 nm) was composed of Vilber Lourmat T-20.L-312 mercury vapor tubes.
Treatment with the HE applicator
The HE technology is provided by the HE applicator attached to the new SurgenTM platform from Pollogen Ltd. A single-use disposable HE tip with 36 micro needles (Gen 36) is attached to the HE applicator for treatment.
The HE novel combination of RF and additional electri-cal energy is aimed at maximizing the treatment effect in order to improve clinical results and stimulate a con-trolled wound-healing response. HE delivery is optimized via the uniform and homogenous penetration of the 36 micro-needles, creating micro-wounds invisible to the eye. The controlled and focused penetration through the epi-dermis, papillary dermis into the reticular dermis allows for optimizing the treatment impact on the dermis while minimizing the visible effect on the epidermis.
The Surgen platform is equipped with a touchscreen dis-playing pre-programed default adjustable power settings of Low, Medium and High. This evaluation was performed using a single HE treatment on UV aged skin fragments with Low or High energy settings (High settings were higher than maximal device range in order to evaluate treatment safety and efficacy using excessive parameters). Untreated UV aged skin fragments served as control.
Analysis methods
Various skin analyses methods were performed at pre-defined intervals:
Histological evaluation
Histological analysis of the epidermis and dermis was performed using H&E (Hematoxylin eosin) staining. A comparison between the effects of low and high energy levels on both affected and un-affected tissue zones was evaluated with an analysis of epidermal modifications (destruction or partial reconstruction) at D0 (a few hours after UV aging and single treatment), D2, D5 and D10.
Histology was performed at different time points in order to investigate the progress of skin response following treat-ment. Evaluations of specific components below were done at D2 and D10 respectively, according to the optimal con-ditions required for each response.
Epidermal mitotic index evaluation
Evaluation of the epidermal mitotic index was performed on D2 using antibody Ki67 (Dako, clone MIB-1, marker cells in the M, S, G1 and G2 phases of the cell cycle). Immuno-detection was completed with an indirect technique of immunoperoxydase in 4 levels, amplified (kit DAKO) and stained in red by AEC (3-amino-9-ethylcarbazole). Results are expressed in % of positive epithelial cells for the 6 donors.
Collagen fibers morphometric evaluation
Morphometric evaluation of collagen fibers was performed on D10 on 4 m thick serial sections that were specifically stained with a picric acid solution containing 0.1% Sirius red. Collagen calculations are performed on the whole slice as it is difficult to identify the treatment impact sites after the red Sirius coloration for the morphometric collagen analysis is applied.
For a quantitative analysis of collagen, a computerized image analysis of each section was performed. The stained slides were examined using a microscope (Leitz) (magnifi-cation ×160) connected to a camera unit (XC-75 CE) and microprocessor (Q520). Collagen bundle areas were mea-sured in m2 and the relative collagen content of the dermis was then expressed as a percentage.
Glycosaminoglycans analysis
Quantification of glycosaminoglycans (GAGs) was per-formed on D10 by using Hale staining. This analysis was effectuated on the skin of 4 donors. A semi-quantitative intensity scoring method of 0-4 was used to evaluate con-centration of GAGs in low and high HE power levels treated skin samples. For each donor, the analysis was performed by evaluating the entire slice in at least 6 -7 zones at mag-nification 40 within the epidermis, superficial and mid to deep dermis. The average of these data was evaluated for each donor and the overall average GAGs was calculated for the 4 donors.
Elastic fiber morphometrical analysis
Quantitative analysis of elastic fibers was performed on D10. Serial sections 4 m thick were obtained and specifi-cally stained with Catechine. This analysis was effectuated on the skin of 4 donors. A computerized image analysis of each section was made. The stained slides were examined using a microscope (Leitz) (magnification ×160) connected to a camera unit (XC-75 CE) and microprocessor (Q520). Elastic fiber area was measured in m2 and the relative elastin content of the dermis was then expressed as a per-centage.
Statistical analysis
Mean values and standard deviations were calculated for each parameter. The statistical significance of data was determined using the Student’s t-test with p<0.05 consid-ered statistically significant.
Results
Histological evaluation
Histological evaluation of the skin demonstrated the differ-ent impacts obtained with the HE applicator using low or high parameters. Impact zones with unaffected intact areas in between were shown; about 5 impacts could be seen at ×40 magnification on the histological slides (skin biopsy was 11 mm in length). A section of a histological slide with 2 impact zones of treatment with high HE parameters is shown in figure 1. Affected epidermis and areas of con-densed dermal collagen are visible directly under the zones of impact.
Figure 2 demonstrates the evolvement of epidermal and dermal modifications following exposure to low and high HE parameters.
In fragments treated with low parameters, at D0 imme-diately after treatment, micro ablation of the epidermis with destruction of the dermal-epidermal junction was present, with the impact extending into the upper dermal layer. For the 6 donors, the mean width of the impact was 221.85 ± 122.9 m, while the depth was 124 ± 85.8 m. With high HE parameters, the size of the epidermal and dermal effects was more prominent. Demarcated zones of ablation and necrosis of the epidermis with destruc-tion of the dermal-epidermal junction and dermis were observed. For the 6 donors, the mean width of the impact was 515.46 ± 424 m, while the depth was 498.3 ± 579.4 m. Moreover, under the crater-shaped abla-tion, zones of condensed collagen were observed with a depth of 200.8 ± 64.5 m. Modifications persisted at D2 and D5 without healing of the epidermis over the treated zone.
At D10, in skin samples exposed to low HE parameters, regeneration of the basal cell layer under the modified epithelial zone was sometimes observed. Following high HE parameters, a new basal cell layer was observed for one donor with the elimination of necrotic epithelium. For the others, the modifications caused by the impact persisted at D10 to a certain extent. These findings were expected in the ex-vivo human skin model, when alterations are prominent,only partial healing process can be observed and we have never observed complete healing, as may be observed in vivo.
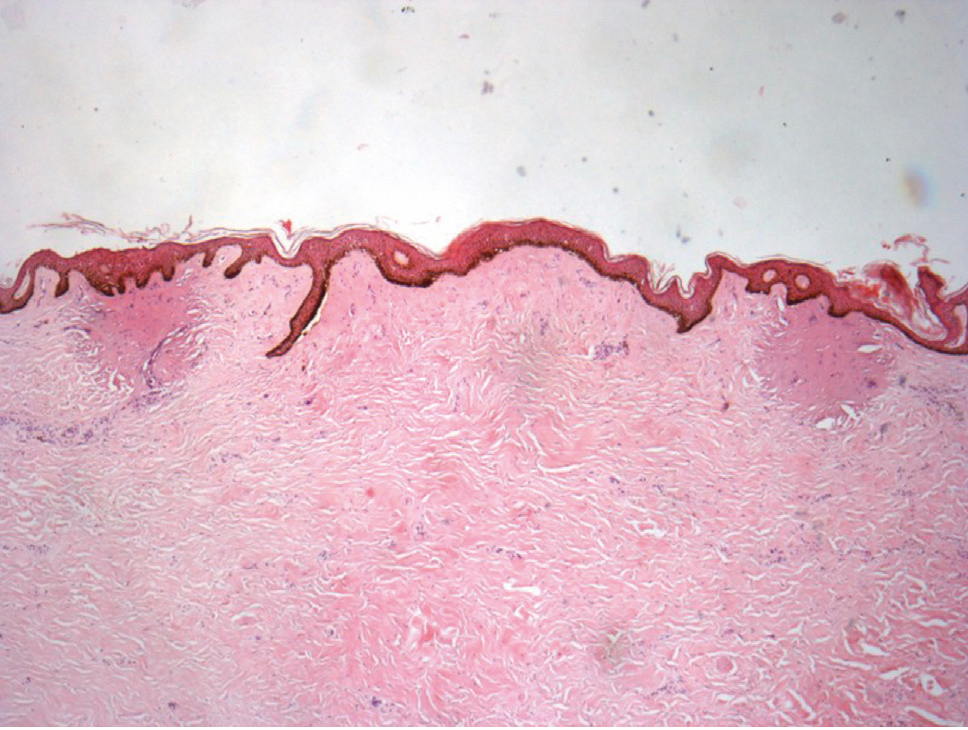
Figure 1. Histology analysis of UV aged skin at D0 after expo-sure to high HE parameters (H&E stain, x40). 2 areas of impact are present with unaffected zone in between.
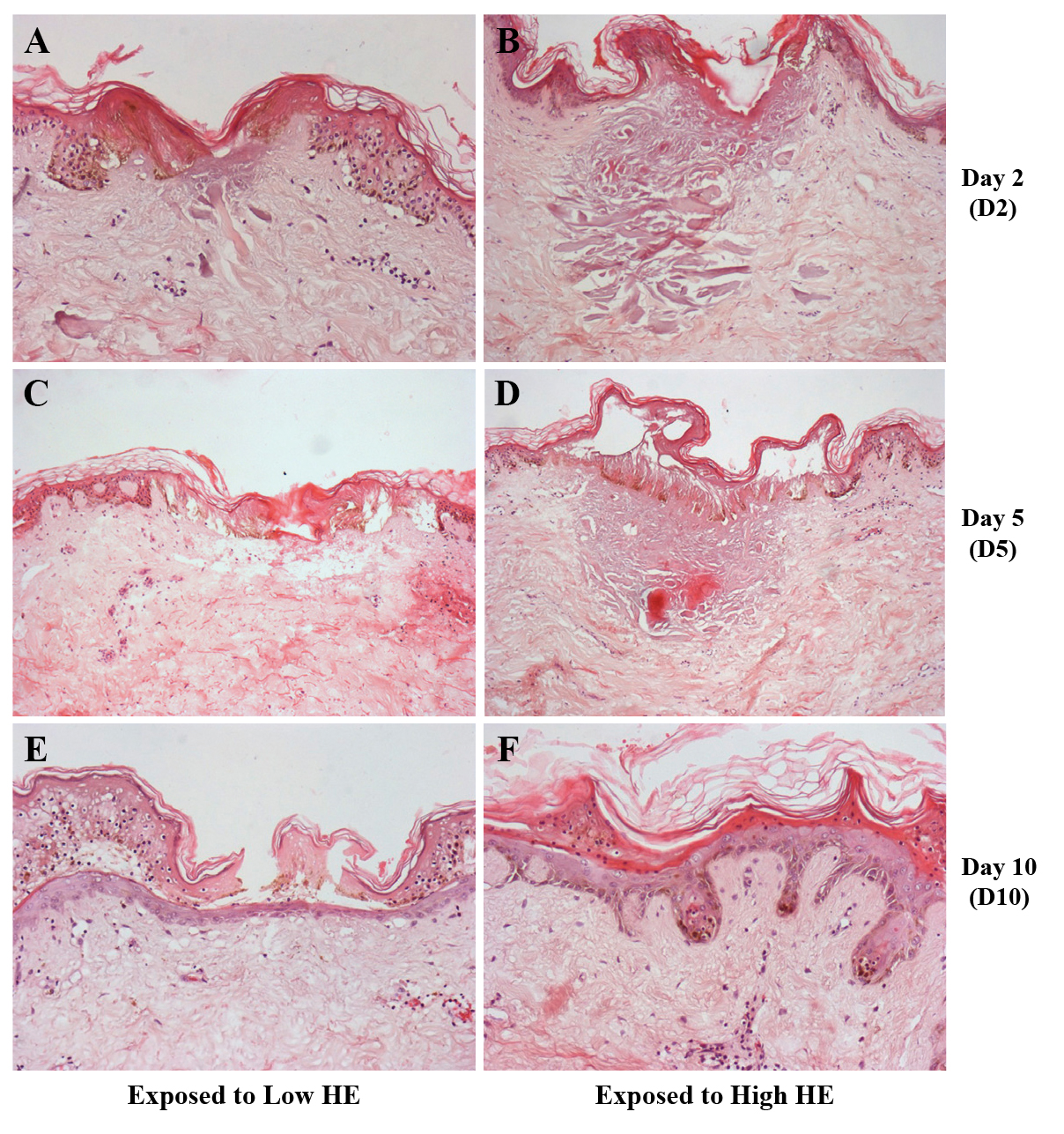
Figure 2. Histological analysis of UV aged skin, demonstrating progress of healing process (H&E stain).
A:UV+LowHEatD2(×100,1cm=66m); B: UV + High HE at D2 (×100,1cm=75m); C: UV + Low HE at D5 (×100); D: UV + High HE at D5 (×100); E: UV + Low HE at D10 (×200); F: UV + High HE at D10 (×200). Micro ablation of the epidermis is noticed with destruction of the dermal-epidermal junction both in Low and High HE. The impact extends into the upper dermal layer, the dermal effect is usually more prominent following High HE exposure (B, D). At D10 (E, F), epithelium regeneration is noticed along with the elimination of necrotic epidermal tissue both in Low and High exposure fragments. In addition, in High HE exposure (F), basal layer regeneration was demonstrated.
Evaluation of epidermal mitotic index
The immuno-detection observed just adjacent to the HE treatment zones on the whole slice (and not in the impact zone itself), revealed a very statistically significant augmen-tation of positive epithelial cells at D2. The percentage of mitotic cells rose from an average of 9.17% in experimen-tally aged skin to 15.52% in the skin exposed to low levels of radiofrequency (p = 0.002) and to 18.73% in the skin treated by HE high levels (p = 0.021).
The results are shown in table 1 and in figure 3. Increase in mitotic index is an indication of the natural wound healing process of re-epithelialization and the repair of damaged tissue in impact areas.
Histological quantification of dermal collagen
Morphometric analysis of collagen at D10 revealed a sig-nificant augmentation from 68.6% average collagen for experimentally aged skin to 75.23% collagen for skin exposed to low levels of HE energy (p = 0.006), and to 76.65% for skin exposed to high levels (p = 0.007). Aug-mentation translates to a 10-11% increase for fragments exposed to Low and High HE levels respectively. It should be noted that calculations are conducted on the whole slices and not on confined treatment impact zones. The results for the histological quantification of dermal collagen are expressed in table 2 and in figure 4.
Table 1. Evaluation of the Mitotic index expressed by % pos-itive cells for antibody Ki67.
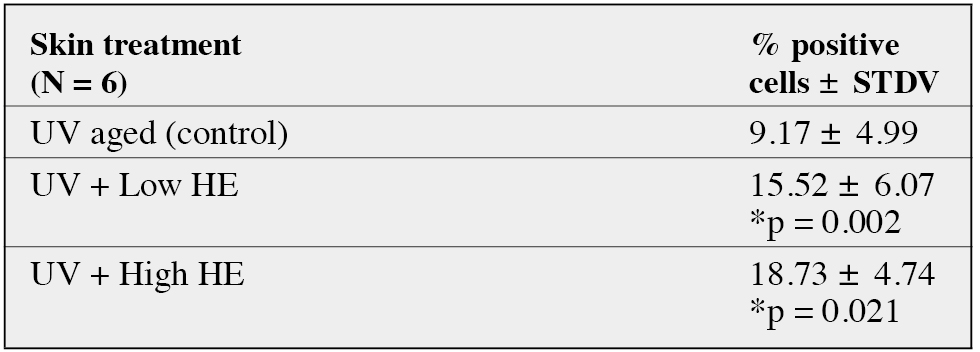
*Statistically significant difference in comparison with control UV aged skin. (Paired Student T test, p<0.05)
mentation translates to a 10-11% increase for fragments exposed to Low and High HE levels respectively. It should be noted that calculations are conducted on the whole slices and not on confined treatment impact zones. The results for the histological quantification of dermal collagen are expressed in table 2 and in figure 4.
Analysis of glycosaminoglycans
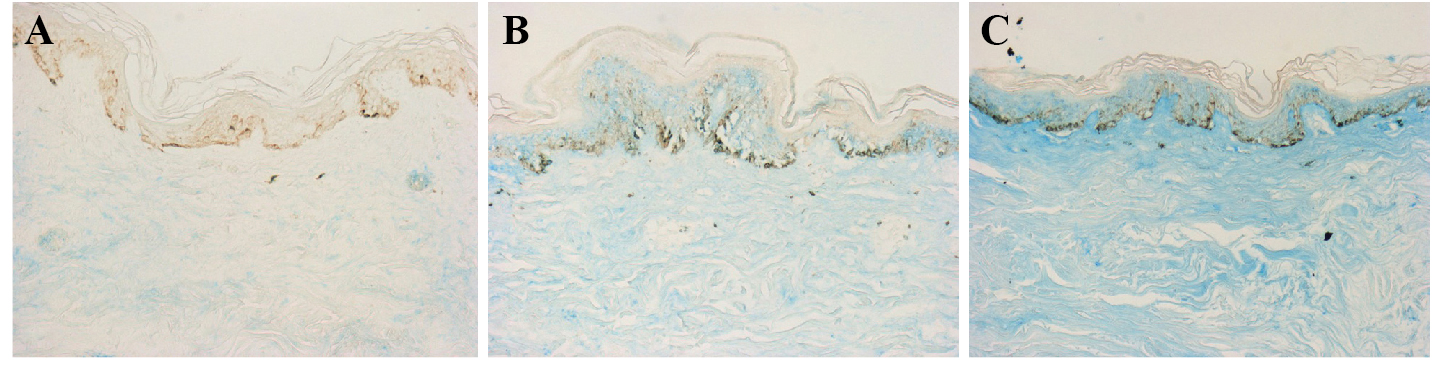
A significant increase in the quantity of glycosaminogly-cans (GAGs) was found, with direct correlation to the level of HE exposure. An augmentation from the average score
Table 2. Histological and morphometric evaluation of colla-gen: % collagen content in the dermis (Sirius red staining) at D10
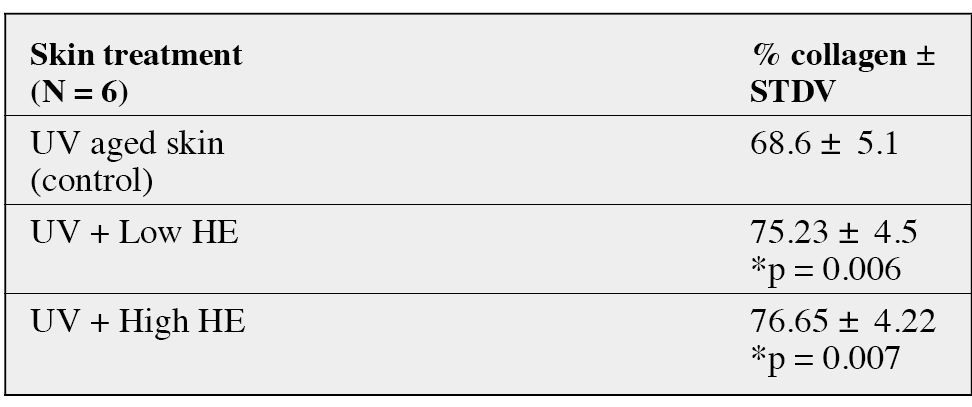
*Statistically significant difference in comparison with control UV aged skin. (Paired Student T test, p<0.05)
of 0.15 GAGs for experimentally aged skin to 0.35 aver-age score was found in the epidermis adjacent to the skin exposed to low levels of HE. Exposure to high levels of HE resulted in a statistically significant increase of GAGs in the epidermis, with an average score of 0.7 (p = 0.04). In the superficial dermis a significant augmentation of aver-age GAGs increased from 1.18 for experimentally aged skin to an average score of 1.93 for skin adjacent to the area exposed to low levels of HE (p = 0.01). Using high lev-els of HE resulted in a statistically significant increase of GAGs in the superficial dermis with an average score of 2 (p = 0.002).
Finally in the mid-deep dermis, a significant augmentation of average GAGs was observed, from 0.5 for experimentally aged skin to an average score of 1.75 for skin adjacent to the area exposed to low levels of HE (p = 0.019). Using high levels of HE resulted in a statistically significant increase of GAGs in the deep dermis with an average score of 1.88 (p = 0.004). Results for the quantification of (GAGs) for 4 donors are expressed in table 3 and in figure 5.
Histological quantification of dermal elastic fibers
Morphometric evaluation of elastic fibers by computerized image analysis, revealed a significant augmentation from 11.18% average for experimentally aged skin to 12.4% for skin exposed to high levels of HE (p = 0.05). Low levels of HE did not show modification of elastic fibers levels.
See also: Microcurrent Facial Toning, RF Skin Device for Home Use, Tripollar Stop V
Discussion
A comparison study, evaluating the effectiveness of surgi-cal face lifts versus a fractional RF micro-needle treatment for improving skin laxity, demonstrated that, even though the outcome following surgery was better, the fractional RF micro needles offered an impressive non-surgical alter-native with the major advantage of absence of scars and minimal downtime [15].
Recent studies have demonstrated effective results and impressive histological findings following fractional RF treatments performed in-vivo and ex-vivo on human skin samples (TriFractionalTM by Pollogen Ltd.) [16]. Histolog-ical analysis of in-vivo treated skin, one day after treatment, showed epidermal necrosis in the involved area and an effect on the papillary as well as upper reticular dermal collagen. One week after treatment, in-vivo histological evaluation demonstrated epidermal regeneration and a dermal effect. Histological analysis results of skin samples exposed to the same fractional RF using an ex-vivo model were in line and further confirmed the in-vivo histological results and demonstrated a significant increase in collagen content. Hantash et al. evaluated the effect of a fractional RF micro needle technology (RenesisTM) on human subjects who were treated immediately, 2 days, 14 days, 28 days, or 10 weeks prior to abdominoplasty [17]. The authors observed
Figure 3. Immunohistochemical analysis of mitotic index at D2 (Ki67, ×200). A significant augmentation of positive epithelial cells is noticed in skin fragment B (UV+Low HE) and in fragment C (UV+High HE) in comparison to the control A (UV).

Figure 4. Analysis of collagen at D10 (Sirius red stain, ×200) UV-aged fragments (A) compared to UV-aged fragments exposed to High HE (B). An increase of collagen fibers in (B) in the dermis is demonstrated under the HE treatment zone.
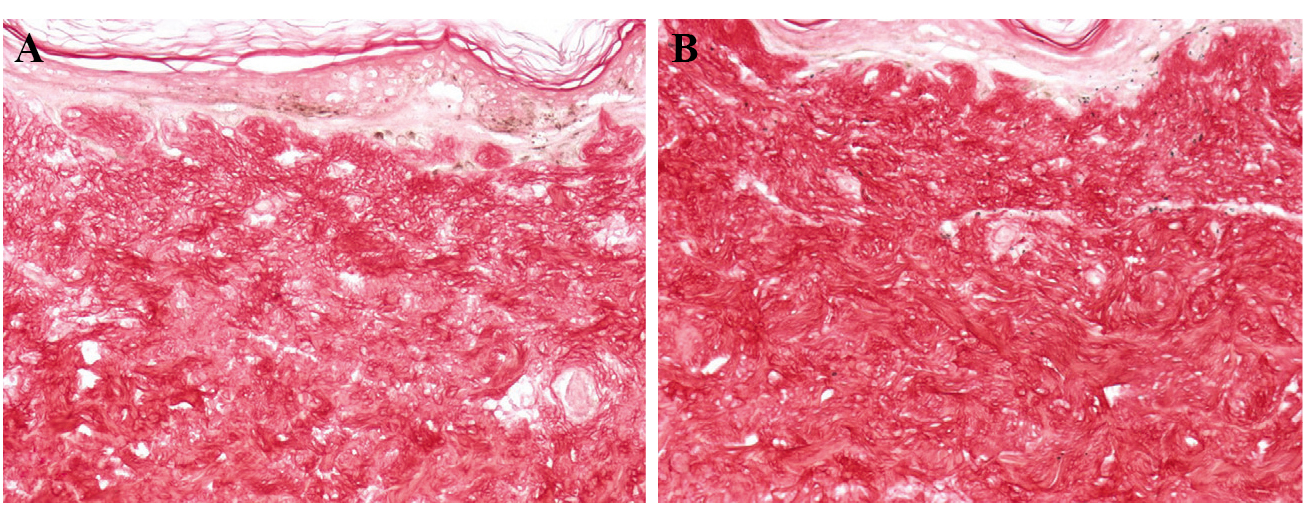
Table 3. Evaluation of GAGs (Hale staining). Analysis performed by measurement of intensity via semi-quantitative scores of 0-4.
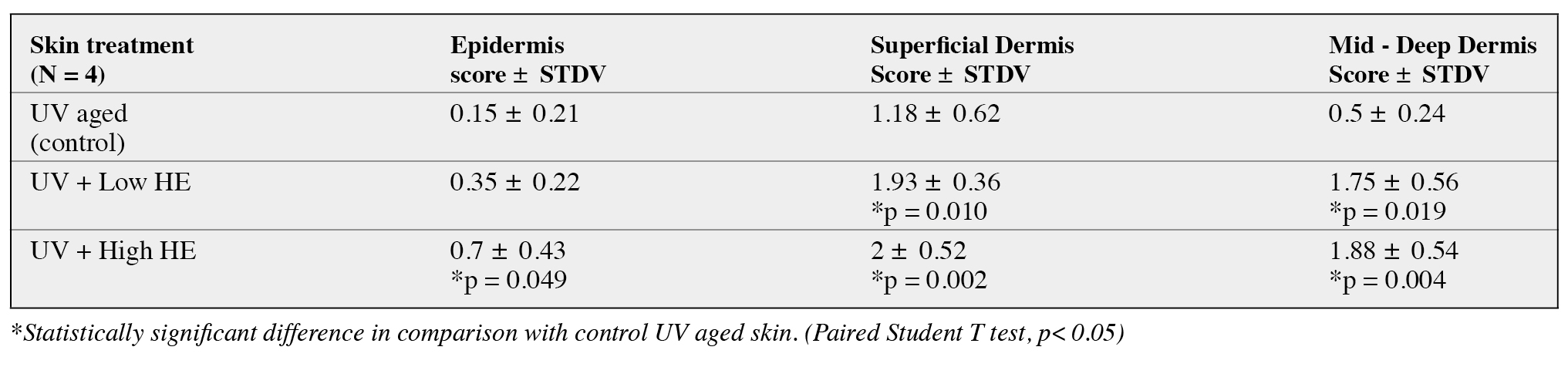
*Statistically significant difference in comparison with control UV aged skin. (Paired Student T test, p<0.05)
Figure 5. Analysis of GAGs at D10 (Hale staining ×200). A: UV aged control; B:UVaged+LowHE C: UV aged + High HE. GAG augmentation is seen in the epidermis and dermis of skin fragments B and C compared to the control fragment A. Exposure to high HE yielded more GAGs than low HE.
a RF thermal zone pattern in the reticular dermis separated by zones of unaffected dermis, with complete sparing of the vasculature as well as dermal structures such as sebaceous glands, hair follicles and sweat glands. The observed ther-mal zones were replaced by new collagen within 10 weeks. The authors also reported an increased volume of the retic-ular dermis along with an increased content of hyaluronic acid and elastin.
In this present ex vivo evaluation we observed a clear pattern of a fractional treatment effect with areas of impact (micro-wounds) surrounded by unaffected tissue, with the depth and size of impact directly correlated to the level of energy used. The High HE level used in this ex vivo experiment is greater than the actual High levels of the HE applica-tor on the Surgen device, this was in order to exaggerate and differentiate the effect of high HE compared to low parameters.
The histological findings of this study demonstrated an effective wound healing process. Even though healing in the ex vivo human skin model is not equivalent to normal healing as observed in vivo, it clearly indicates the pattern of the biological process that occurs in the human body. An increase of the mitotic index indicates a positive response of wound healing and the generation of new epidermal cells, hence leading to skin renewal and rejuvenation post resur-facing. Recovery of the basal lamina layer was noticed in some fragments, in addition to re-epitheliazation in a few fragments (which is not necessarily expected in the ex vivo model). All fragments exposed to HE demonstrated a signif-icant increase in collagen compared to UV-aged unexposed fragments demonstrating neocollagenesis following expo-sure to HE. An increase in GAGs was noticed in the dermis and epidermis of treated fragments, with higher levels of GAGs in skin exposed to high HE. This is expected, as GAGs, which include hyaluronic acid, are an important component of wound recovery, serving a multifaceted role in the various stages of healing [18]. Hyaluronic acid, which is the most prominent GAG in the skin, acts as an early pro-moter of the inflammation stage of wound recovery and, during the granulation phase, it facilitates cell migration by providing a hydrated matrix. Next, during re-epithelization, it is associated with the proliferation of basal keratinocytes and, finally, during the remodeling stage, hyaluronic acid is a major component of the cellular matrix, reducing fibrous scaring. It is important to note that, during the stage of collagen restructuring, the increase in GAG content may also indicate an increase of other GAGs, such as chon-droitin sulphate. Additional tests using methods to directly and specifically analyze hyaluronic acid content are rec-ommended to further support the current findings and the significance of the GAG increase [19, 20].
These histological findings demonstrate an expected wound repair process resulting in the elimination of necrotic epi-dermal tissue and renewed epidermal and dermal tissue, with increased dermal collagen density and GAGs. These findings indicate that HE technology can be safe and effec-tive for skin resurfacing, reduction of wrinkles and for the improvement of lax skin.
Conclusions
This ex-vivo model of human skin maintained in survival condition allowed us to demonstrate the ability of the new HE fractional technology to rejuvenate the skin via con-trolled micro wounds that induce epidermal renewal and dermal regeneration through a demonstrated healing pro-cess. Furthermore, this study demonstrated the difference in effect between low and high parameters, showing the efficacy of controlled injury at both levels as a significant increase in the mitotic index, collagen density, elastic fibers and GAGs was observed in both treated groups of skin
fragments.
Disclosure. Financial support: A research grant for the study was provided by Pollogen Ltd, the study sponsor. Conflict of interest: none.
1. El-Domyati M, Attia S, Saleh F, et al. Intrinsic aging vs photoaging:A comparative histopathological, immunohistochemical, and ultrastruc-tural study of skin. Exp Dermatol 2002; 11: 398-405.
2. Fisher GJ, Varani J, Voorhees JJ. Looking older: Fibroblast collapse and therapeutic implications. Arch Dermatol 2008; 144: 666-72.
3. Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: nonablative fractional and ablative laser resur-facing. J Am Acad Dermato 2007; 58: 719-37.
4. Tanzi EL, Alster TS. Side effects and complications of variable pulsed erbium: YAG laser skin resurfacing: extended experience with 50 patients. Plast Reconstr Surgery 2003; 111: 1524-9.
5. Nanni CA, Alster TS. Complications of CO2 laser resurfacing: an evaluation of 500 patients. Dermatol Surg 1998; 24: 315-20.
6. Willey A, et al. Complications of Laser Dermatologic Surgery. Lasers Surg Med 2006; 38: 1-15.
7. Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Frac-tional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med 2004; 3:426-38.
8. Laubach HZ, Tannous Z, Anderson RR, Manstein D. Skin responses to fractional photothermolysis. Lasers Surg Med 2006; 38: 142-9.
9. Halachmi S, Orenstein A, Meneghel T, Lapidoth M. A novel frac-tional micro-plasma radio-frequency technology for the treatment of facial scars and rhytids: A pilot study. J Cosmet Laser Ther 2010; 12:208-12.
10. Hruza G, Taub AF, Collier SL, Mulholland SR. Skin Rejuvenation and Wrinkle Reduction Using a Fractional Radiofrequency System.J Drugs Dermatol 2009; 8: 259-65.
11. Berube D, Renton B, Hantash BM. A Predictive Model of Minimally Invasive Bipolar Fractional Radiofrequency Skin Treatment. Lasers Surg Med 2009; 41: 473-8.
12. Mulholland1 RS, Ahn DH, Kreindel M, Paul M. Fractional Ablative Radio-Frequency Resurfacing in Asian and Caucasian Skin: A Novel Method for Deep Radiofrequency Fractional Skin Rejuvenation. J Cos-met Dermatol Sci Appl 2012; 2: 144-50.
13. Boisnic S, Branchet-Gumila MC, Benslama L, Le Charpentier Y,Arnaud-Battandier J. Long term culture of normal skin to test the effi-cacy of a hydroxy acid-containing cream. Eur J Dermatol 1997; 7:271-3.
14. Boisnic S, Branchet-Gumila MC, Nocera T. Comparative study of the anti-aging effect of retinaldehyde alone or associated with pretoco-pheryl in a surviving human skin model submitted to ultraviolet A and B irradiation. Int J Tissue React 2005; 27: 91-9.
15. Alexiades-Armenakas M, Rosenberg D, Renton B, Dover J, Arndt K. Blinded, Randomized, Quantitative Grading Comparison of Mini-mally Invasive, Fractional Radiofrequency and Surgical Face-lift to Treat Skin Laxity. Arch Dermatol 2010; 146: 396-405.
16. Levenberg A, Gat A, Boisnic S, Branchet MC. Treatment of Wrinkles and Acne Scars Using the TriFractional, A Novel Fractional Radiofrequency Technology – Clinical and Histological Results. J Cos-met Dermatol Sci Appl 2012, Published Online September 2012.(http://www.SciRP.org/journal/jcdsa).
17. Hantash BM, Ubeid AA, Chang H, Kafi R, Renton B. Bipolar Fractional Radiofrequency Treatment induces Neoelastogenesis and Neocollagenesis. Lasers Surg Med 2009; 41: 1-9.
18. Chen WYJ, Abatangelo G. Functions of Hyaluronan in Wound Repair. Wound Repair Regen 1999; 7: 2.
19. Manuskiatti W, Maibach HI. Hyaluronic Acid and Skin Wound Healing and Aging. Int J Dermatol 1996; 35: 539-44. 20. Parthiba B, Gupta P.D. Cutaneous wound healing-Significance of proteoglycans in scar formation. Curr Sci 2000; 78.






