

Improvement of wrinkles and skin tightening using TriPollar® radiofrequency with Dynamic Muscle Activation (DMA™)
Abstract
Background: Radiofrequency (RF) energy promotes skin renewal by inducing tissue remodeling through dermal heating and neocollagenesis. (See Pollogen’s Stop V Skin Renewal Device)
Aim: To evaluate the safety and effectiveness of a medical esthetic system that com-bines simultaneously TriPollar® RF energy with Dynamic Muscle Activation (DMA™) for improving facial skin tightness and wrinkles.
Methods: A prospective, open-label study. Eleven subjects (mean age, 43 years; Fitzpatrick skin type II-IV) with Fitzpatrick Elastosis Scale (FES) score 3-6 were treated. The participants underwent six weekly treatments. Effectiveness of the treatments was evaluated at 1 and 3 months follow-ups after the last treatment, using the FES and evaluator- and subject-rated Global Aesthetic Improvement Scale (GAIS). Treatment safety and tolerance were evaluated as well. Pain was evaluated on a visual analog scale (VAS) of 0-10.
Results: Treatment was safe, with minimal pain (VAS score less than 1), no adverse events, and no downtime. At 1 and 3 months follow-up evaluation, mean physi-cian-rated FES statistically significantly improved from baseline (4.63 ± 0.88) by 2.27 ± 0.45 for both time points (P < .0001). According to investigator GAI scale at 3 months follow-up evaluations, 81.8% of patients were improved and 18.2% were much improved in fine lines, wrinkles and skin tightness.
Conclusions: Treatment with RF TriPollar® combined with DMA™ is effective and well-tolerated treatment for improving skin tightness and reducing wrinkles.
K E Y WO R D S
DMA™, Dynamic Muscle Activation, facial rejuvenation, radiofrequency, skin tightness, TriPollar®, wrinkles
See also Pollogen’s Eye Wrinkle Reduction Device, Face Slimming Device, Home Facial Device, Geneo Oxypods
1 | INTRODUC TION
Various aging processes lead to skin laxity. Chronological aging of dermal fibroblasts causes a gradual decline in extracellular matrix components of the dermis, such as hyaluronic acid collagen and elas-tic fibers. In addition, extrinsic skin aging, caused by long-term ex-posure to wind, pollution and ultraviolet radiation, repetitive muscle movements (eg, frowning and squinting), and various lifestyle habits such as smoking, sleeping, or diet are characterized by upper dermis elastosis, destruction of its fibrilar structure, increased intercellular substance, and moderate inflammatory infiltrate.1,2 As a result, the support and volume of dermal structures are decreased, leading to reduced skin torsion extensibility and causing wrinkling of the over-lying epidermis.3
The superficial musculo-aponeurotic system (SMAS) is a contin-uous, organized fibrous network connecting the facial muscles with the dermis. It comprises a three-dimensional scaffold of fat cells, elastic fibers, and collagen fibers.4 The SMAS envelops and supports facial tissues. Due to aging, SMAS becomes less elastic, weakening this skin support frame. Therefore, treatment of aging skin should also involve re-contouring of the SMAS.5
Multiple technologies exist for rejuvenating the skin and reduc-ing the signs of aging. These include ablative and nonablative lasers at various wavelengths, intense pulsed light, photodynamic therapy, high-intensity focused ultrasound (HIFU), electrical stimulation, and radiofrequency (RF) energy.6-9
RF energy has been used for tissue ablation and hemosta-sis in surgical applications for many years. In the last 20 years, utilization of RF has also gained popularity in esthetic applica-tions, due to its ability to induce tissue remodeling, skin tight-ening, and improvement of wrinkles through dermal heating and neocollagenesis.10-12
The novel treatment of noninvasive TriPollar® RF energy with Dynamic Muscle Activation (DMA™) targets several layers of tis-sue and muscle for the treatment of wrinkles and laxity. The first component, TriPollar® RF, comprises three or more electrodes that deliver RF energy into the skin at a frequency of 1 MHz and a maximum power of 50 W. This component produces volumetric heating of the dermal tissue through rapidly oscillating electro-magnetic fields that cause movement of charged particles within the dermis and generation of heat that is proportional to the tis-sue’s electrical resistance.13 The second component is DMA™ technology, applied by transcutaneous electrical muscle stimu-lation that causes internal muscle contraction to tone and firm muscles.14
The two components can work separately or simultaneously at the same treatment.
TriPollar® RF-based systems have shown effectiveness in treat-ing cellulite, reducing abdominal and thigh circumference,12,13,15 reducing striae distensae,16 and improving facial skin tightness and wrinkles.12,13,17,18
In this study, we evaluated the safety and effectiveness of the use of TriPollar® RF and DMA™ for facial skin tightening and im-provement of wrinkles.
2 | MATERIALS AND METHODS
2.1 | Design and subjects
This was a single center, prospective, open-label, intra-individual controlled trial. The study was approved by the Institutional Review Board (IRB). All of the participants signed an informed consent form prior to the treatment course.
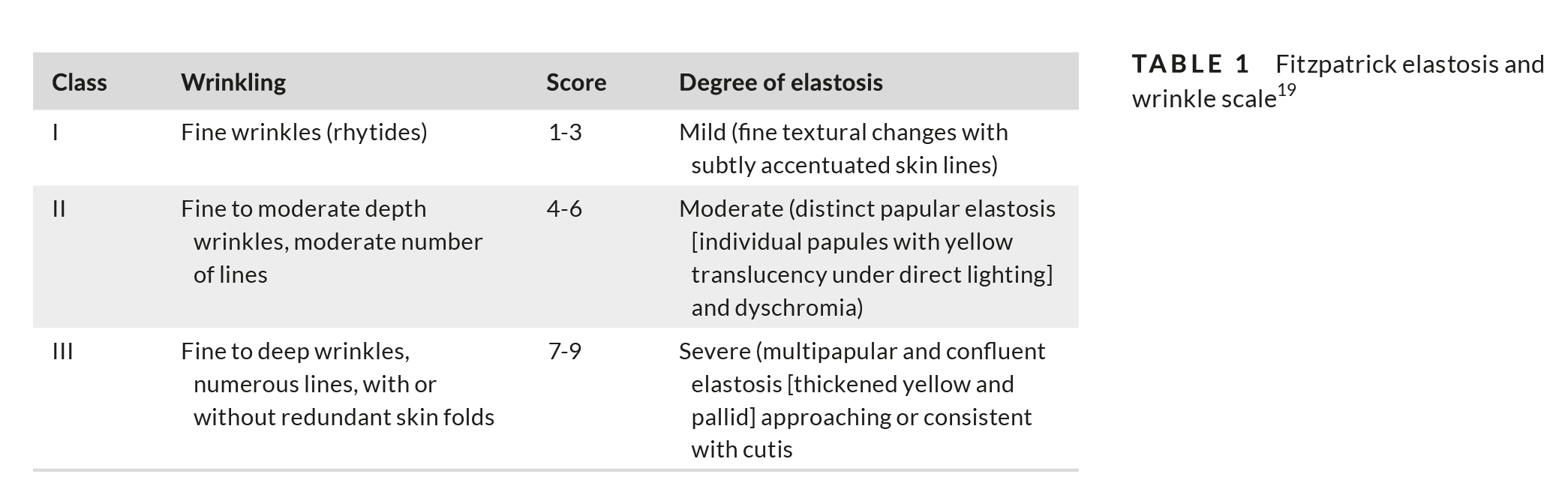
Healthy adult subjects, 30-50 years of age with Fitzpatrick Skin Type I-VI and with Fitzpatrick Wrinkle Classification score 3-6 (Table 1),19 were included in the study. Exclusion criteria included pregnancy or breastfeeding, any implantable electronic device that could be disrupted by RF energy, severe concurrent conditions or an impaired immune system or specific esthetic implants or treatments in the treated area prior to the study.
2.2 | Treatment protocol and settings
The treatment area included the entire face as well as the perioral and periorbital regions. The subjects received six treatments, at 1-week intervals with follow-up visits at 1 and 3 months after the last treatment. Prior to each treatment, the treatment area was thor-oughly cleaned and dried. The treatment area was lubricated with medical-grade glycerin (87% or higher purity).
2.2.1 | Treatment parameters
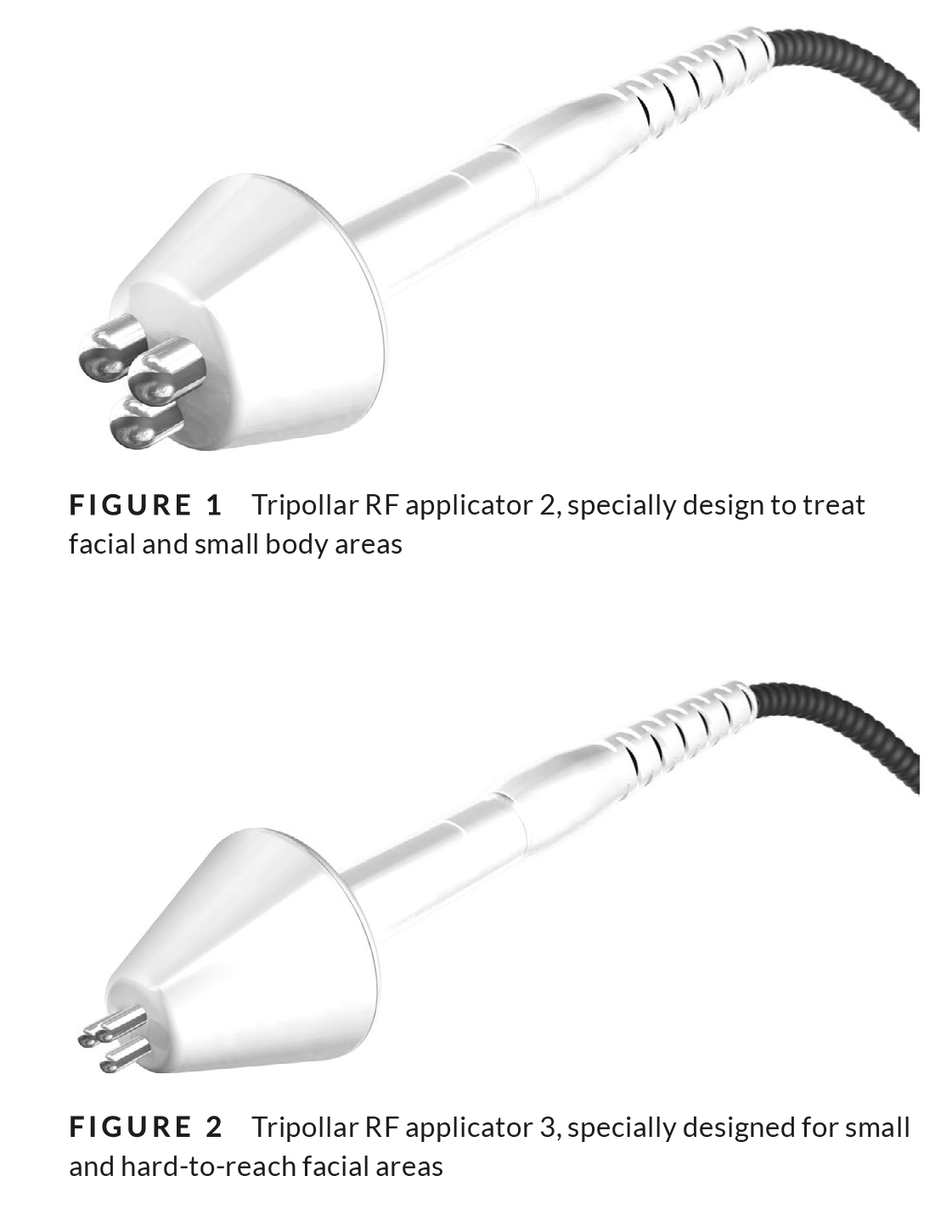
The treatments were performed using Legend+ system by Pollogen. All six treatments were conducted using default parameters’ level, which were then gradually increased according to the subject’s sen-sation and feedback (Table 2). First, the entire face was treated with Tripollar RF applicator 2 (Figure 1), specially design to treat facial and small body areas, the periorbital and perioral areas were treated with Tripollar RF applicator 3 (Figure 2), which was specially designed for small and hard-to-reach facial areas afterward the jawline was treated with DMA™.
The DMA™ component has 3 adjustable parameters: DMA height (power/amplitude), DMA width (contraction time), and DMA

frequency (contractions per second). Treatment started with default parameters and increased gradually according to patient’s comfort. First, the DMA height was increased or decreased to the level pleas-antly tolerated by the patient. Then, the pulse width was increased and then if needed, the frequency.
Muscle activation sensation was monitored verbally throughout the treatment according to patient sensation and feedback.
2.3 | Study end points and outcome measures
The primary end point of the study was the success rate at the 3 months follow-up visit, with success defined as an improvement of at least one point on the FES assessed by investigator as compared to baseline. The secondary end point of the study was skin improve-ment on the FES at the 3 months follow-up visit as compared to baseline. Additional end points were as follows: investigator-rated improvement of skin texture according to the Global Aesthetic Improvement Score (GAIS), FES improvement by blinded evaluators from “before and after” photographs at 3 months follow-up, subject-rated skin improvement, subject satisfaction, and downtime.
At baseline and at the 1 and 3 months follow-up visits, the treat-ment area was photographed with a digital camera at standardized conditions.
The investigator and subjects independently graded the skin’s improvement by comparing the subject’s visual appearance at fol-low-up against an archival photograph taken at baseline. Evaluator-rated change in skin texture and wrinkles was evalu-ated by the FES.
The GAIS scale was used independently by the investigator, blinded evaluators and the subjects for grading the change in skin appearance from baseline to the follow-up visits at 1 and 3 months after the last treatment (0 = worse, 1 = no change, 2 = improved, 3 = much improved, and 4 = very much improved).
Pain experienced during the treatment was reported by the sub-jects on a visual analog scale (VAS) ranging from 0 (no pain) to 10 (intolerable pain).
Treatment safety was assessed by the incidence of treat-ment-related skin response, any adverse events that occurred fol-lowing the treatments, and by the duration of downtime (defined as the period of time following the procedure during which the subject had edema and erythema and felt unable or unwilling to go out in public).
The subjects’ satisfaction rate with the treatment outcome was recorded at the 1 and 3 months follow-up visit on the following scale: none, slight, moderate, good, and very good.
2.4 | Statistical analysis
Statistical analyses were mainly descriptive in nature, with continu-ous variables summarized by mean and standard deviation, and cat-egorical variables by count and percentage. The difference between baseline and follow-up was analyzed using paired t test with a one-tailed distribution. The level of significance was 5%.
3 | RESULTS
A total of 11 subjects (ten females and one male) with a mean age
of 43.0 ± 4.3 years and Fitzpatrick skin types II-IV were included in the study. The majority of subjects were Caucasian (10/11, 90.9%),
and one subject was Asian. Baseline physician-assessed FES was
4.64 ± 0.88.
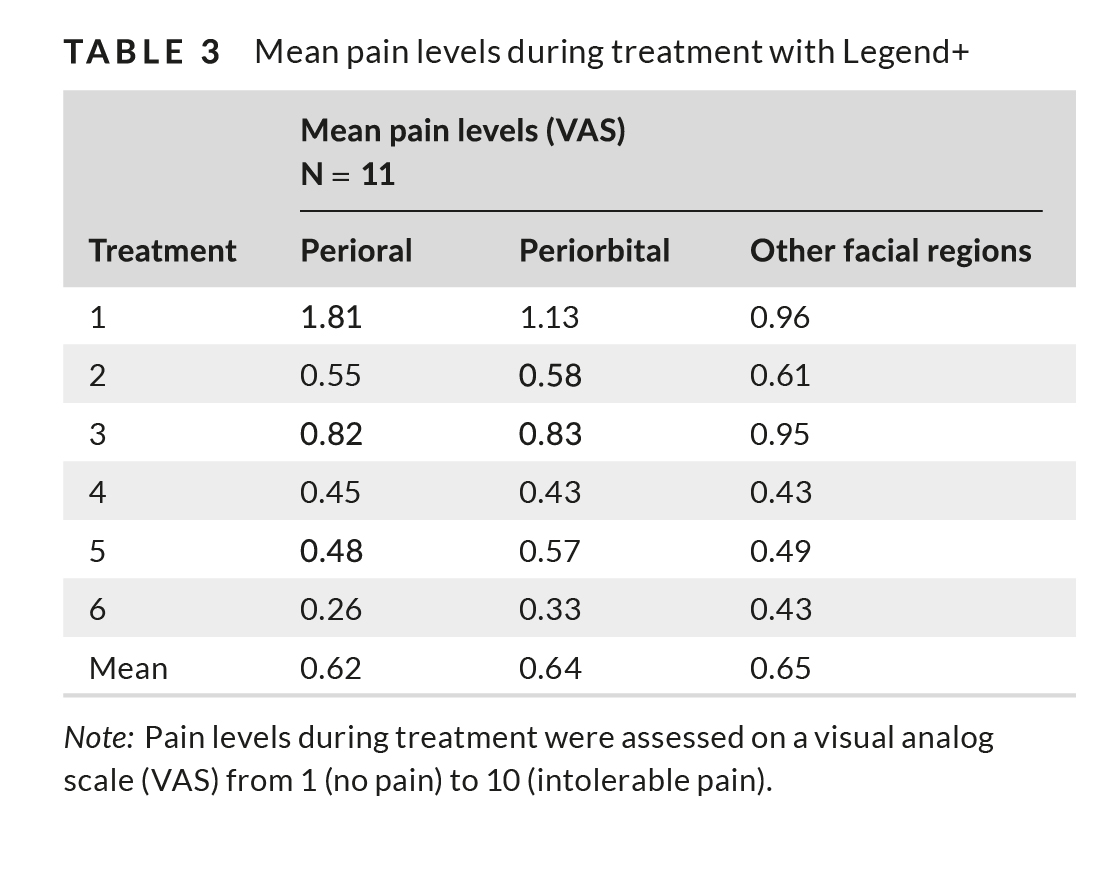
Mean pain levels for all 6 treatments were minimal in all of the treated facial regions: 0.62, 0.64, and 0.65 for the perioral, perior-bital, and the rest of the face, respectively (VAS scale 0-10, Table 3). When assessing pain levels by treatment, mean pain levels were greatest during the first treatment session and decreased during the course of treatment, down to a minimum at the sixth (and last) treat-ment session.
No adverse events or downtime were reported for any of the subjects following any of the treatments.
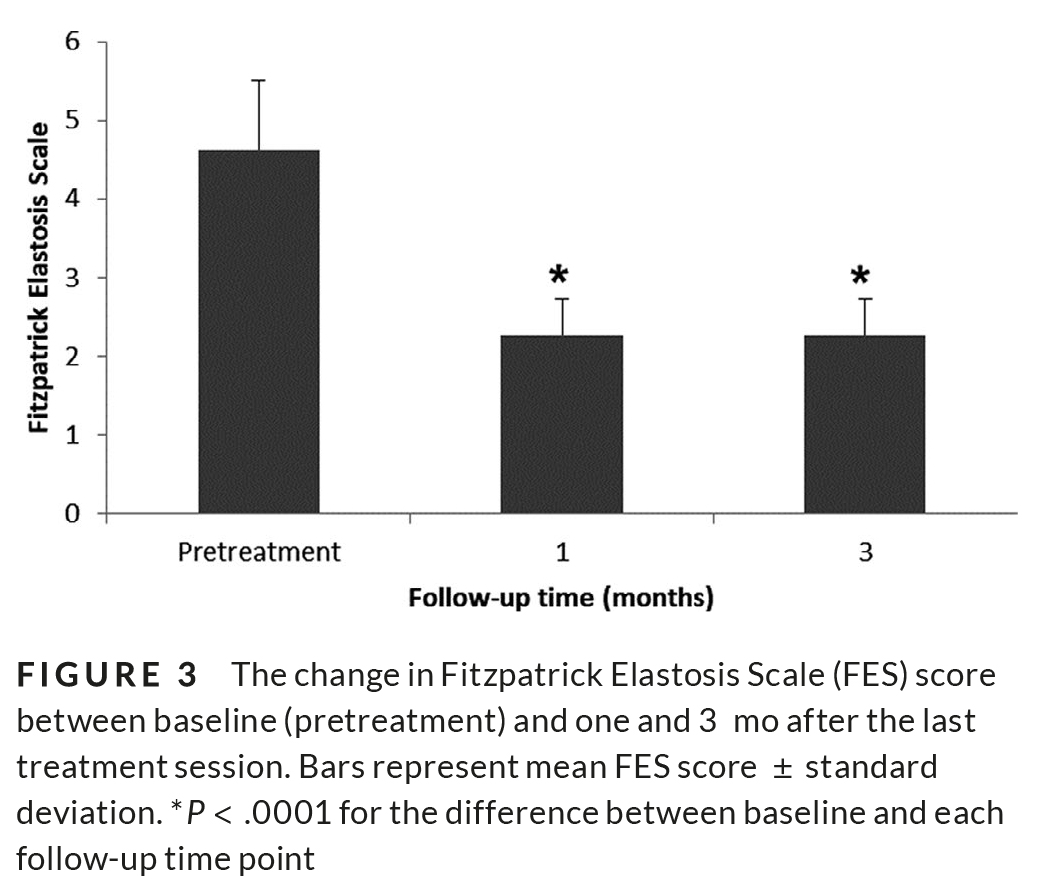
One and three months after the last treatment session, mean physician-rated FES was greater than one point and statistically significantly improved from baseline by 2.27 ± 0.45 for both time points (P < .0001, Figure 3).
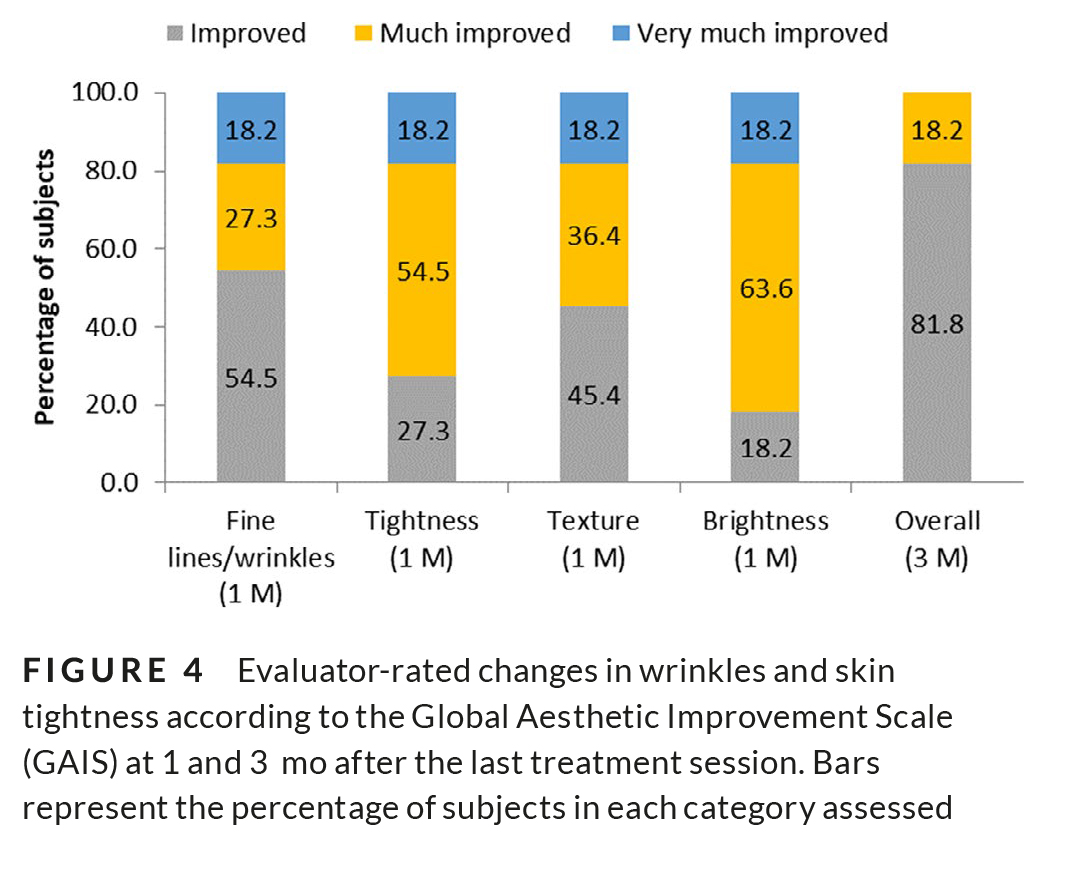
One month after the last treatment session, fine lines and wrin-kles were noted as “improved” in 54.5% of subjects, “much improved” in 27.3%, and “very much improved” in 18.2%. At the same follow-up time point, skin tightness was noted as “improved” in 27.3% of subjects, “much improved” in 54.5%, and “very much improved” in 18.2%. Skin texture was noted as “improved” in 45.4% of subjects, “much improved” in 36.4%, and “very much improved” in 18.2%. Brightness was noted as “improved” in 18.2% of subjects, “much improved” in 36.4%, and “very much improved” in 18.2% (Figure 4). Three months after the last treatment session, investigator-rated overall improvements in fine lines, texture, tightness, and brightness according to the GAIS were noted as “improved” in most subjects (81.8%) and “much improved” in 18.2% of them (Figure 2).
Blinded evaluation of the “before and after” photographs at the 3 months follow-up showed a mean reduction of 1.27 points in FES from baseline. Representative “before and after” photographs of study participants are shown in Figure 5.
Over a third of the subjects (37%) reported that skin tightness was “improved”-“much improved” after the first treatment. Ninety-one percent (91%) of subjects reported moderate to very good im-provement in the appearance of their cheeks after four treatments.
After five treatments, all 11 subjects reported slight to very good overall improvement in appearance.
According to the subject satisfaction questionnaires, 90.9% of patients reported various degrees of improvement 3 months follow-ing the treatment course.
4 | DI SCUSS ION
This study has shown that six consecutive treatments with the novel TriPollar® RF with DMA™ for the treatment of facial wrinkles and skin tightening, significantly improved skin elastosis and wrinkles as seen at 1 and 3 months after the last treatment session. A third of the subjects reported skin tightening already after the first treat-ment, and all of the subjects reported improvement in the appear-ance of their skin after five treatments.
Our findings corroborate other reports on improvements fol-lowing the use of TriPollar® RF and DMA™ technologies on facial
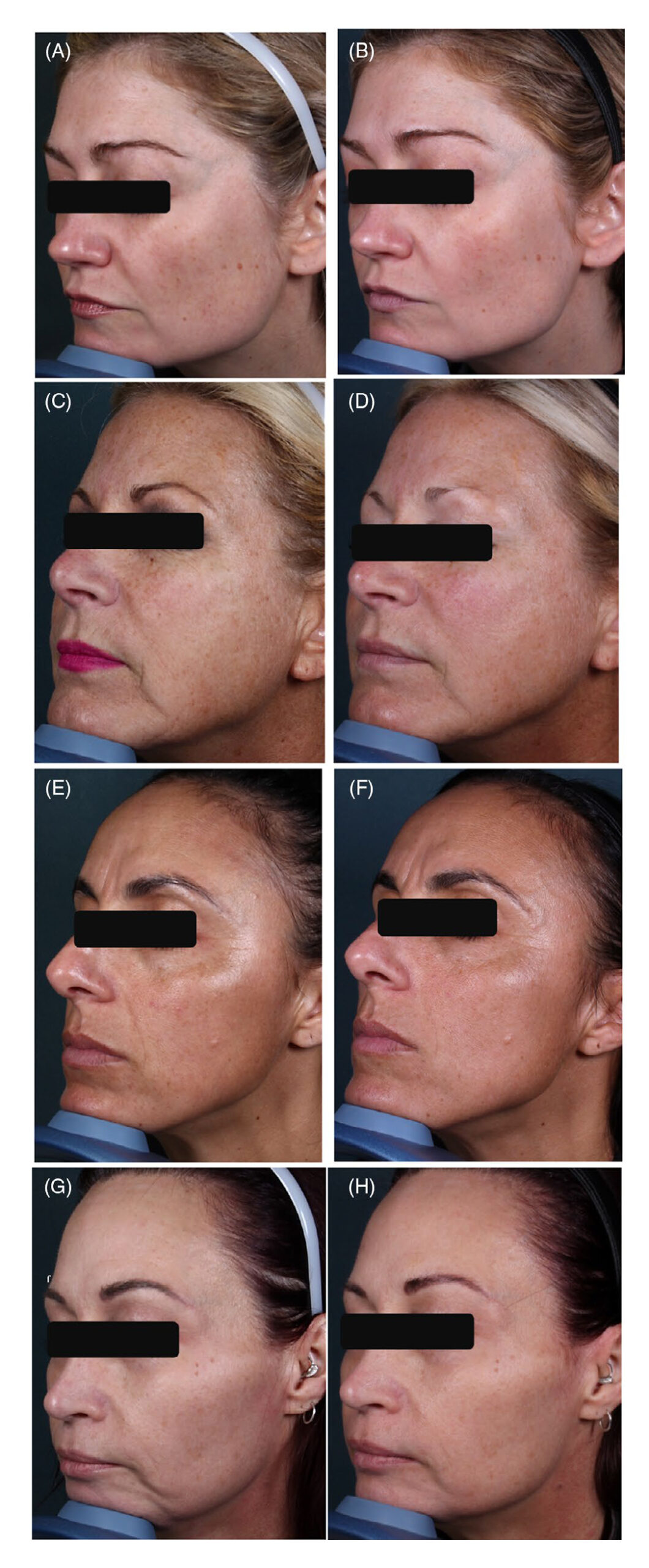
FI GUR E 5 Representative “before and after” photographs of study participants. A 37-y-old female patient, before (A) and 3 mo after six treatments sessions (B). Significant improvements were noted in skin tightness, nasolabial folds, and marionette lines. A 49-y-old female patient, before (C) and 3 mo after six treatments sessions (D). Significant improvements were noted in skin tightness, fine lines, and wrinkles. A 45-y-old female patient, before (E) and 3 mo after six treatments sessions (F). Significant improvements were noted in skin tightness, nasolabial folds, and skin texture. A 47-y-old female patient, before (G) and 3 mo after six treatments sessions (H). Significant improvements were noted in skin tightness and wrinkles
wrinkles. The use of TriPollar® RF together with DMA™ for facial wrinkles was also reported by Potekaev and Zhukova in a study that included 20 women (mean age, 43 years) that were treated for fa-cial wrinkles with the TriPollar® and DMA™ technologies weekly for 8 weeks. Significant improvements in thickness and elasticity (lifting effect) of tissue, and facial skin color homogeneity were noted as well as reduced sharpness of mimic and static wrinkles. Ultrasound assess-ment of the skin showed significant dermal-epidermal thickening and increased dermal density.17 Levenberg et al14 showed that subjects who underwent facial treatments using two TriFractional™ skin re-surfacing treatments spaced 1 month apart, with two TriPollar® RF combination with DMA™ 2 weeks after each TriFractional™ treat-ment, improved acne scars, skin texture, and wrinkles together with facial contouring. Thus, using DMA™ to restore contour of the SMAS helps strengthen the skin’s support. Other studies reported treatment of facial wrinkles with the TriPollar® RF component alone. In a study that evaluated the improvement in facial wrinkles and rhytides in 37 women (mean age, 52.8 years) that received 8 weekly treatments with TriPollar® RF, improvement was noted in 94%-97% of study partici-pants.18 Levenberg reported an improvement of perioral and perior-bital wrinkles in 9 women treated with TriPollar® RF technology.12 The biological mechanism involved in skin tightening using TriPollar® RF technology included stimulation of dermal fibroblasts with increased collagen synthesis and focal thickening of collagen fibers.13,20
All of the studies above noted that treatment was painless or involved minimal pain. Some of the studies reported post-treatment transient mild-moderate erythema and/or slight edema.12,13,17,18 In the study described herein, treatment was well tolerated, with no adverse skin reactions or adverse events. Pain was minimal, decreas-ing even more with subsequent treatments.
In the current study, mean improvement in wrinkles and skin tightness assessed by FES remained the same at 1 and 3 months after the last treatment session and all of the subjects showed im-provement in wrinkles and skin tightness at the last time point as-sessed (3 months). Maintenance of treatments every 3-6 months is advised due to the natural and continuous aging process.
ACKNOWLEDGMENTS
Dr Michael H. Gold is a consultant and preforms research for Lumenis.
CONFLICT OF INTEREST
Dr Michael H. Gold is a consultant and preforms research for Lumenis.
REFERENCES
1. Farage MA, Miller KW, Elsner P, Maibach HI. Intrinsic and extrinsic factors in skin ageing: a review. Int J Cosmet Sci. 2008;30(2):87-95.
2. Tsatsou F, Trakatelli M, Patsatsi A, Kalokasidis K, Sotiriadis D. Extrinsic aging: UV-mediated skin carcinogenesis.Dermatoendocrinology. 2012;4(3):285-297.
3. Zhang S, Duan E. Fighting against skin aging: the way from bench to bedside. Cell Transplant. 2018;27(5):729-738.
4. Ghassemi A, Prescher A, Riediger D, Axer H. Anatomy of the SMAS revisited. Aesthetic Plast Surg. 2003;27(4):258-264.
5. Marten TJ. High SMAS facelift: combined single flap lifting of the jawline, cheek, and midface. Clin Plast Surg. 2008;35(4):569-603, vi–vii.
6. Gold MH. The future of non-invasive rejuvenation technology: de-vices. J Drugs Dermatol. 2017;16(6):s104-s107.
7. Gutowski KA. Microfocused ultrasound for skin tightening. Clin Plast Surg. 2016;43(3):577-582.
8. Philipp-Dormston WG. Photodynamic therapy for aesthetic-cos-metic indications. G Ital Dermatol Venereol. 2018;153(6):817-826.
9. Asiran Serdar Z, Aktas Karabay E, Tatliparmak A, Aksoy B. Efficacy of high-intensity focused ultrasound in facial and neck rejuvena-tion. J Cosmet Dermatol. 2019;19(2):353-358.
10. Arnoczky SP, Aksan A. Thermal modification of connective tissues: basic science considerations and clinical implications. J Am Acad Orthop Surg. 2000;8(5):305-313.
11. Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. Lasers Surg Med. 2004;34(2):91-97.
12. Levenberg A. Clinical experience with a TriPollar radiofrequency system for facial and body aesthetic treatments. Eur J Dermatol. 2010;20(5):615-619.
13. Kaplan H, Gat A. Clinical and histopathological results follow-ing TriPollar radiofrequency skin treatments. J Cosmet Laser Ther. 2009;11(2):78-84.
14. Levenberg A, Gat A, Christine Branchet M, Boisnic S. Treatment of wrinkles and acne scars using the TriFractional, a novel frac-tional radiofrequency technology—clinical and histological results. J Cosmet Dermatol Sci Appl. 2012;02:117-125.
15. Manuskiatti W, Wachirakaphan C, Lektrakul N, Varothai S.Circumference reduction and cellulite treatment with a TriPollar radiofrequency device: a pilot study. J Eur Acad Dermatol Venereol. 2009;23(7):820-827.
16. Manuskiatti W, Boonthaweeyuwat E, Varothai S. Treatment of striae distensae with a TriPollar radiofrequency device: a pilot study. J Dermatolog Treat. 2009;20(6):359-364.
17. Potekaev N, Zhukova O. Evaluation of safety and efficacy of the Maximus™ system for facial wrinkles. J Cosmet Dermatol Sci Appl. 2013;3(2):151-156.
18. Shapiro SD, Eros Y, Abrahami Y, Leviav A. Evaluation of safety and efficacy of the TriPollar technology for treatment of wrinkles. Lasers Surg Med. 2012;44(6):453-458.
19. Fitzpatrick RE, Goldman MP, Satur NM, Tope WD. Pulsed carbon dioxide laser resurfacing of photo-aged facial skin. Arch Dermatol. 1996;132(4):395-402.
20. Boisnic S, Branchet MC. Ex vivo human skin evaluation of local-ized fat reduction and anti-aging effect by TriPollar radio frequency treatments. J Cosmet Laser Ther. 2010;12(1):25-31.






