

ORIGINAL RESEARCH REPORTS
Evaluation of safety and efficacy of the TriFractional RF technology for treatment of facial wrinkles
Abstract
Introduction:Skin resurfacing is an accepted gold standard for the treatment of skin laxity, photodamage, and appearance of visible lines and wrinkles. However, the relatively signifi cant risk and the long downtime associated with whole area resurfacing treatments have led to the introduction of fractional resurfacing lasers and radiofrequency (RF) technologies. This study was performed in order to evaluate the safety and effi cacy of the new TriFractional technology using the 3F Applicator (A3F), designed to enable skin resurfacing and treatment of wrinkles using fractional RF energy. Methods: Thirty-two subjects were recruited in two sites and were treated with the A3F for the reduction of facial wrinkles and followed for 3 months after the last treatment. The safety of using the TriFractional system was established by the physicians ’ assessments and observations of adverse events after each treatment. To evaluate treatment effi cacy, subject ’ s pretreatment and posttreatment digital images were assessed and graded by two blinded uninvolved physicians based on Fitzpatrick Wrinkle and Elastosis scale. Results: No signifi cant adverse side effects were detected or reported. Evaluation of photographs of study subjects at baseline and 3 months follow-up by the two blinded physicians, revealed improvement (downgrade of at least 1 score according to the Fitzpatrick scale) in 80% and 73% of subjects as graded by the two revie-wers. Study subjects reported no pain to moderate pain during treatment with no need of pain relief medication beyond topical anesthesia. The majority of study subjects (83.3%) noted that treatment results met their expectations to different extent levels, and most of study subjects (70%) indicated that they will recommend the A3F treatment to their friends. Conclusions: The results of this study clearly indicate that the TriFractional technology using the 3F applicator provides a safe, tolerable, and effective treatment of facial wrinkles.
Introduction
Skin laxity, photodamage, appearance of visible lines and wrinkles, and an overall decline in skin texture are typical characteristics of aging human skin (1). An increased demand for aesthetic treatments for enhancing appearance has led to the development and introduction of a myriad of technologies and treatment options. Skin resurfacing has been shown to be highly effective for improving a wide variety of aging skin symptoms, resulting in epidermal renewal and a better organized and newer dermal matrix. Numerous methods are available for skin resurfacing, including chemical peels, dermabrasion, lasers, and recently fractional RF (2).
Continuous wave carbon dioxide (CO 2 ) lasers were first introduced for skin resurfacing in the mid-1980s as an alternative to chemical peels. However, due to many adverse effects associated with this technology, short-pulse, focused-beam CO 2 lasers, in addition to erbium-doped yttrium aluminum garnet lasers (Er:YAG) were introduced, which remove skin in a precisely controlled manner, enabling impressive clinical results for treatment of photodamaged and ageing skin. Unfortunately, full skin laser resurfacing technologies are associated with prolonged healing, signifi cant down time, and high complication rates, particularly in darker skin patients, due to the fact that the entire epidermis and papillary dermis are removed, often over large skin areas such as the entire face (3,4).
To overcome the complications and risks associated with full skin resurfacing, a new generation of fractional laser resurfacing technologies was intro-duced in 2003 (Solta Medical, Hayward, CA), open-ing a window to safer, faster healing skin resurfacing options (5,6). Rather than treating an entire skin sur-face, the fractional laser treats a condensed matrix of small “ islets ” of tissue leaving intact skin in-between these islets. The unaffected intact “ islets ” enable an immediate healing process of the treated surface, reducing downtime, and risk of complications. Many fractional laser systems have since been introduced and cleared for marketing worldwide, mostly based on CO 2 and Er:YAG laser technology (7 – 9). Over the past decade, Radiofrequency (RF) has become a well-established energy for noninvasive aesthetic treatments of face and body (10 – 12). In the past several years, fractional RF resurfacing tech-nology has been introduced and has become an accepted method for skin resurfacing.
Similar to fractional laser skin resurfacing, frac-tional RF systems allow controlled fractional skin resurfacing with minimal downtime in a safe man-ner. Fractional RF systems affect the epidermal layer, inducing an effective micro-ablative skin resur-facing while simultaneously enhancing the dermal layer. The combined effect results in an improved appearance of wrinkles, fi ne lines, and acne scars (13). The novel TriFractional approach using the new A3F applicator from Pollogen ® is designed to enable fractional skin resurfacing for treatment of wrinkles along with skin enhancement via controlled epidermal micro-ablation and concomitant dermal remodeling (14).
The current study was conducted in order to evaluate the effi cacy and safety of the TriFractional technology using the A3F for treatment of facial wrinkles (see also: skin and face rejuvenation). Clinical evidence is provided to demon-strate A3F treatment safety and effi cacy.
Methods
The study was conducted in two centers in the USA: Tennessee Clinical Research Center Inc., Nashville, TN and Research Across America, Plano, TX. The study was approved by Independent IRB, Inc, Plantation, FL.
A total of 32 subjects were recruited to the study after signing an Informed Consent and meeting all inclusion/exclusion criteria.
Exclusion criteria included pregnancy or breast-feeding, any implanted electronic device, any active dermatological or collagen or vascular disorders, history of skin cancer, prolonged intake of medication that can affect healing, tendency to keloid scaring, any severe concurrent conditions, metal implants in treated area (not including dental implants), and specifi c aesthetic procedures in the treatment area prior to the study.
Subjects received three treatments, spaced
3 weeks apart, with A3F for improvement of wrin-kles, and were followed 1 and 3 months after the last treatment.
Prior to each treatment and at each follow-up visit, the treatment area was assessed visually and photographed at standardized conditions using high-resolution digital photography for producing high-quality images, for enabling accurate assessment of wrinkle improvement by blinded evaluators.
Technology
The TriFractional applicator (A3F) is indicated for skin resurfacing and for the treatment of wrinkles by means of micro-ablation and coagulation. A dispo-sable treatment tip, containing a matrix of bipolar tiny electrodes, is attached to the distal end of the applicator and is placed on the skin for treatment. RF current is delivered sequentially between each of the pin electrodes and the large electrodes which sur-round the pin matrix. Due to this design, a relatively high RF power density is generated in the tissue under each electrode, resulting in fractional treat-ment microwounds in the epidermis, which is in direct contact with the electrodes while heat is deliv-ered deeper into the dermis. This fractional manner of energy delivery leaves intact zones in between the directly affected areas that serve as a reservoir of healthy cells to promote a faster, more effective wound healing. The A3F emits a “ train ” of three sub-pulses with a very short Thermal Relaxation Time (TRT), in one treatment pulse. This modality enables an enhanced effect of deeper penetration and opti-mized effi cacy, with less discomfort to the patient and a deeper gradual thermal effect. Shortly after treatment, there is moderate skin erythema and edema in the treated zone, which resolves within 1 – 3 days. During the healing phase, small pin-point epi-dermal crusts may appear at each micro-ablated spot which exfoliate naturally after a few days leading to mild epidermal resurfacing.
Visits and treatments
Prior to treatment, the treated area was cleaned and dried thoroughly and a topical anesthetic agent was applied (Emla, AstraZeneca, Wilmington, DE), according to manufacturer guidelines.
The A3F was placed on the skin with slight pres-sure to ensure good contact, in areas with uneven skin surface; the treatment area was slightly “ stretched ” before placing the applicator. During the fi rst treatment of all subjects, the low parameters program was used. At following treatments, high parameter programs were used, according to indi-vidual skin condition, subject ’ s needs, and skin response. Immediately after the treatment, the treated area was visually assessed for skin responses, includ-ing edema and erythema and responses were docu-mented. Subjects were instructed to avoid exposure to the sun and to apply sunblock daily.
Follow-up visits were intended for assessing the treated area and for acquiring subjects ’ photographs. At the last (3 months) follow-up visit, subjects were asked to rate level of satisfaction from the cosmetic improvement by fi lling out a satisfactory question-naire and the investigators were asked to fi ll in a general questionnaire evaluating the technology and an individual questionnaire evaluating the improve-ment of each subject.
See also: Oxygeneo skin tightening, Geneo X Facial Treatment Device
Study end points
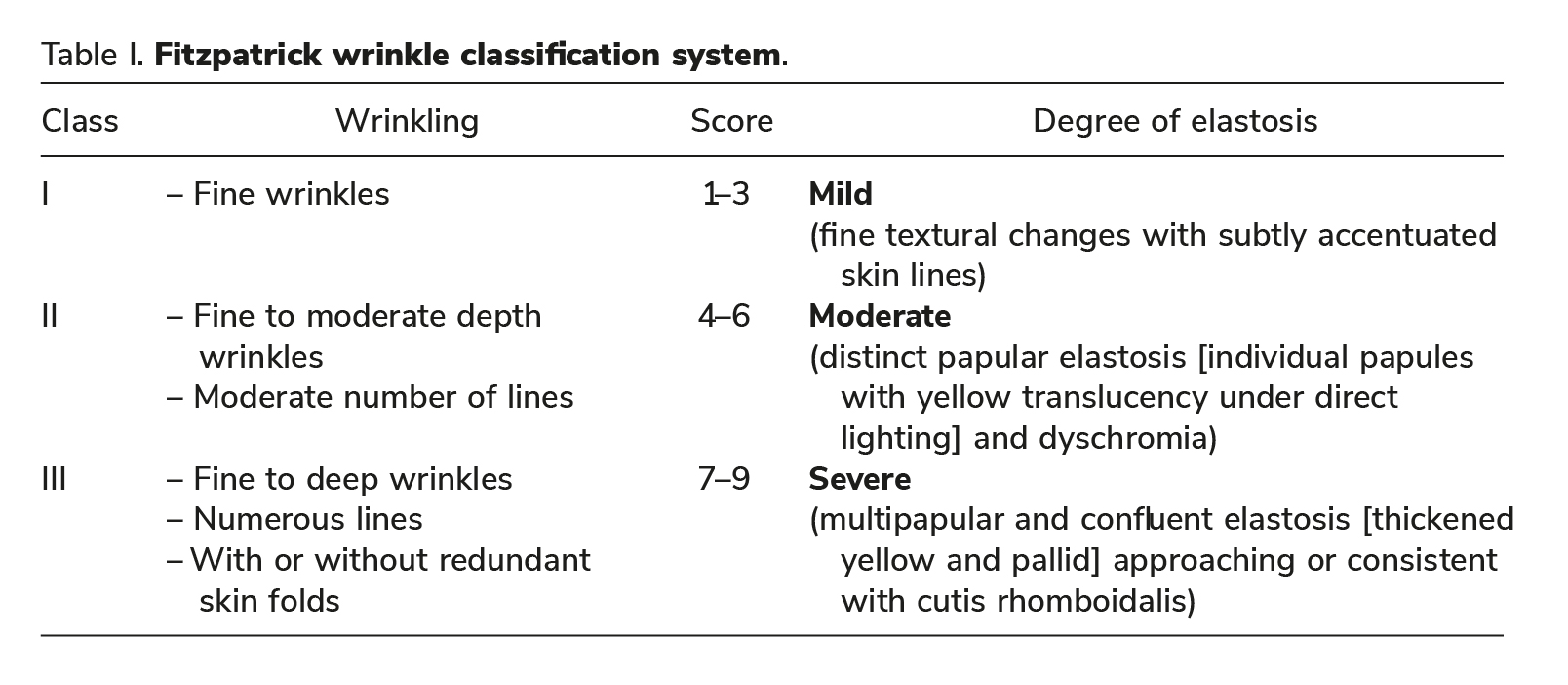
For treatment effi cacy evaluation, baseline and 3 months follow-up photographs of each subject were randomly presented and scored by two independent physicians (blinded evaluators) using the Fitzpatrick Wrinkle and Elastosis scale (Table I) (15).
Scores of baseline and 3 months follow-up pho-tographs were compared.
Success of subject ’ s treatment was defi ned as a downgrade of at least 1 score according to the Fitz-patrick Scale at 3 months follow-up compared to that of baseline.
In addition to the effi cacy evaluation established by the blinded evaluators, each Principal Investigator (PI) visually inspected and graded each subject using the Fitzpatrick Wrinkle and Elastosis scale at baseline and at 3 months follow-up visit.
Safety of the procedure was determined by mon-itoring any occurrence of adverse effects or compli-cations directly related to the treatment, during or after the treatment.
Subject satisfaction was gathered from subject ’ s questionnaires completed at 3 months follow-up. Investigators ’ satisfaction from treatment results of each subject was gathered from the investigator questionnaires.
Results
Thirty-two healthy subjects were recruited to the study (30 females and 2 males), ages 40 – 64 (Mean age 51.227.31 years), and Fitzpatrick skin type 2 – 5. Of the 32 subjects recruited, 30 subjects who completed the full study course and were followed to the 3 months follow-up were included in efficacy evaluation. One subject withdrew consent after two treatments due to work schedule; an additional subject was lost to follow-up. One of the 30 subjects who completed the study course and included in efficacy evaluation underwent only two A3F treatments due to personal constraints. For assessing safety of the A3F, results of all 32 subjects who were treated were used.
Treatment safety
The data of all 32 subjects who underwent treatment were analyzed. As expected, mild to moderate erythema and several cases of mild edema (fi ve cases, 16%) were detected at the site of treatment, all cases resolved without treatment, within a few hours. In most cases, scabs appeared within several days (aver-age 2.53 1.15) and lasted several days (average 5.63 2.3). Three mild related adverse effects were reported during the study (hyper pigmentation; red-ness, and acne break out), all three cases resolved spontaneously within 1 – 2 months. There were no incidences of infections, scarring, hypopigmentation, or any other serious complications. Treatments were well tolerated with minimal to no pain by the majority of study subjects (75%; 62%, and 58% of study subjects, at the fi rst, second and third treatment, respectively). None of the subjects needed any additional analgesic or other pain medication during treatment.
Treatment efficacy
Treatment efficacy was determined by objective evaluation of photographs taken at baseline (prior to treatment initiation) and at the 3 months
follow-up, by two blinded physicians who arbitrarily (non-chronologically) scored the photos using the Fitzpatrick Elastosis Scale. The results of 30 subjects who completed the study course were included in the effi cacy analysis.
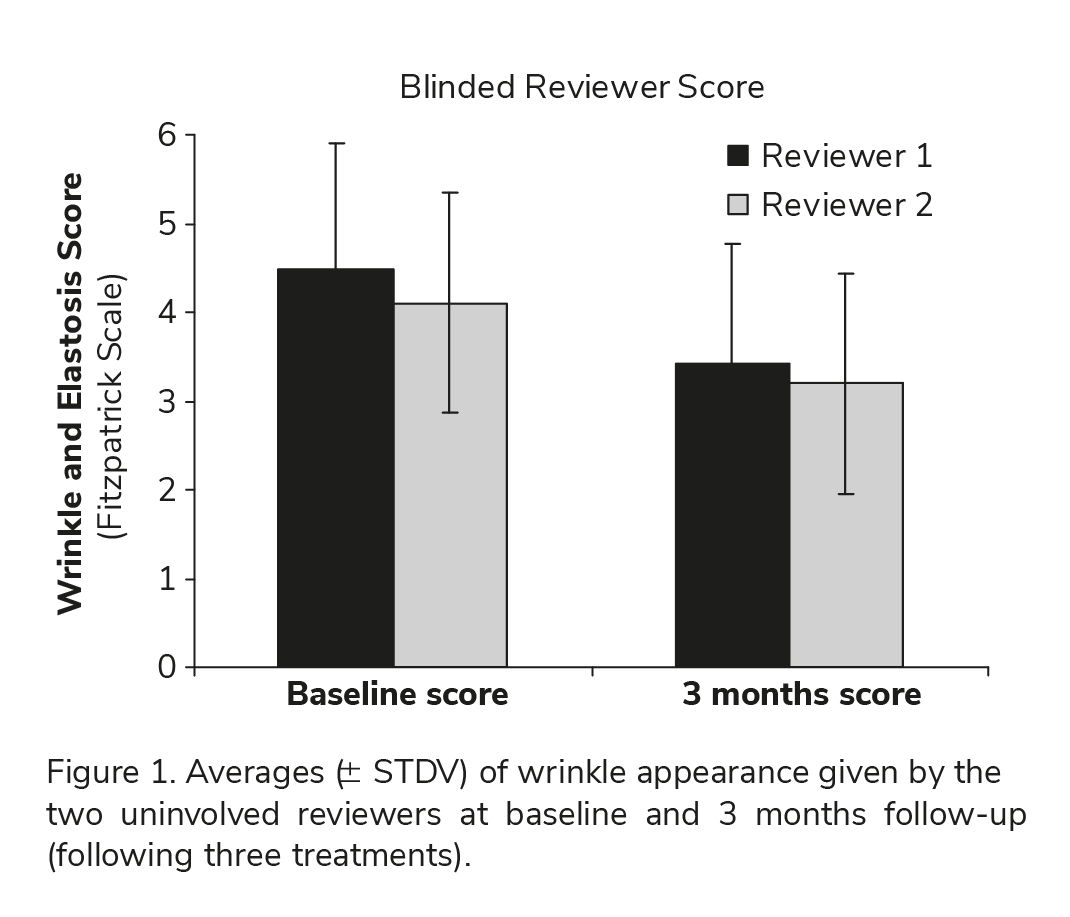
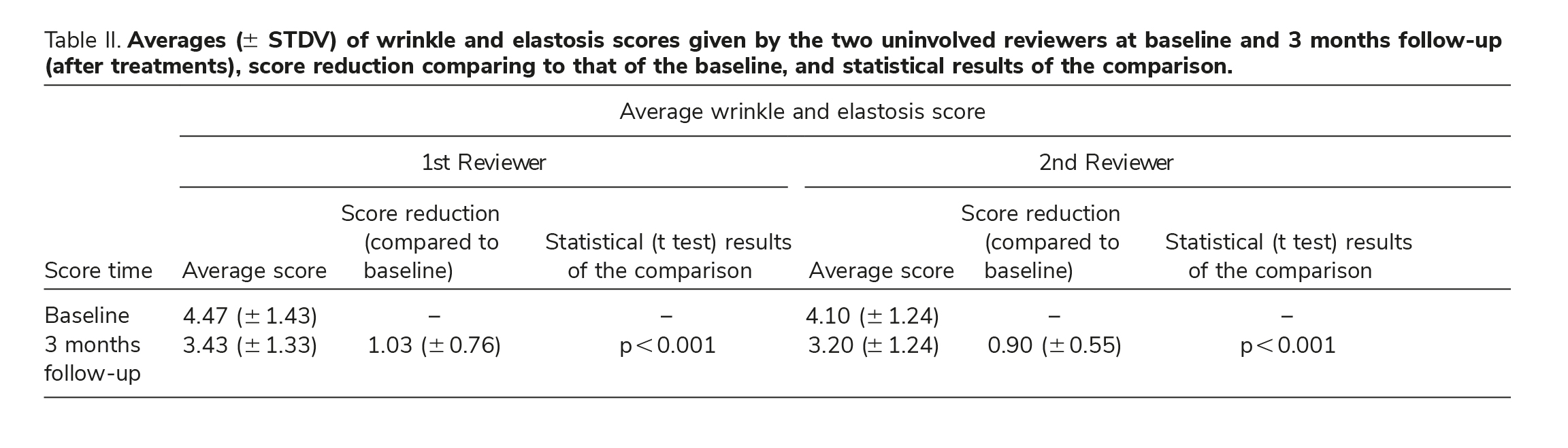
Analysis revealed an improvement in wrinkle appearance in the majority of study subjects (80% according to one reviewer and 73.3% according to the second reviewer). Score differences were found to be statistically signifi cant (p 0.001) for both reviewers, further indicating treatment effi cacy. Table II and Figure 1 represent averages ( STDV) of Fitzpatrick scores given by the two reviewers at baseline and 3 months follow-up.
In order to evaluate level of agreement between the two uninvolved physicians, statistical comparison (using two-sided paired t test) was conducted between the baseline wrinkle and elastosis score pro-vided by the two blinded reviewers. The statistical analysis failed to reveal signifi cant differences (p 0.05) between the baseline wrinkle score of the two reviewers. Furthermore, same result was obtained while comparing the 3 months follow-up scores of the two reviewers. The statistical comparison of the 3 months follow-up wrinkle and elastosis score, obtained by the two uninvolved evaluators, indicates no statistical difference (p 0.05) between the two reviewers. These results indicate that both uninvolved reviewers were in agreement regarding wrinkle and elastosis degree, at baseline as well as at 3 months follow-up, enhancing the study results. Table II sum-marizes the uninvolved physicians score at baseline and 3 months follow-up.
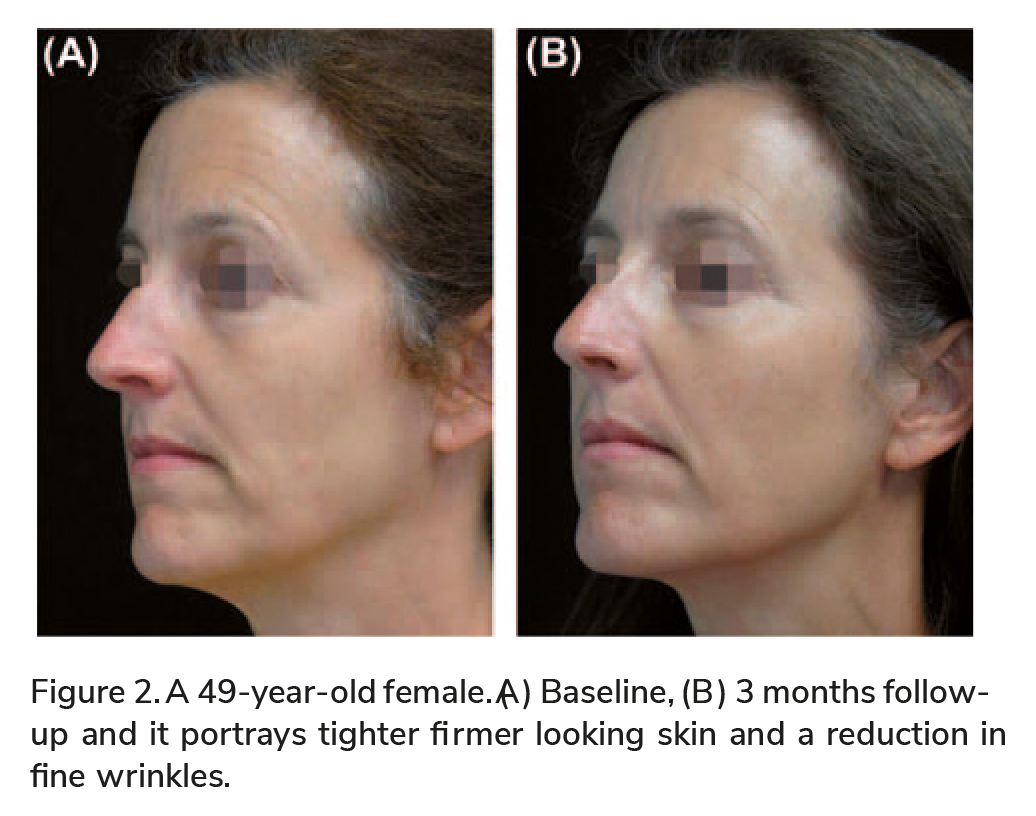
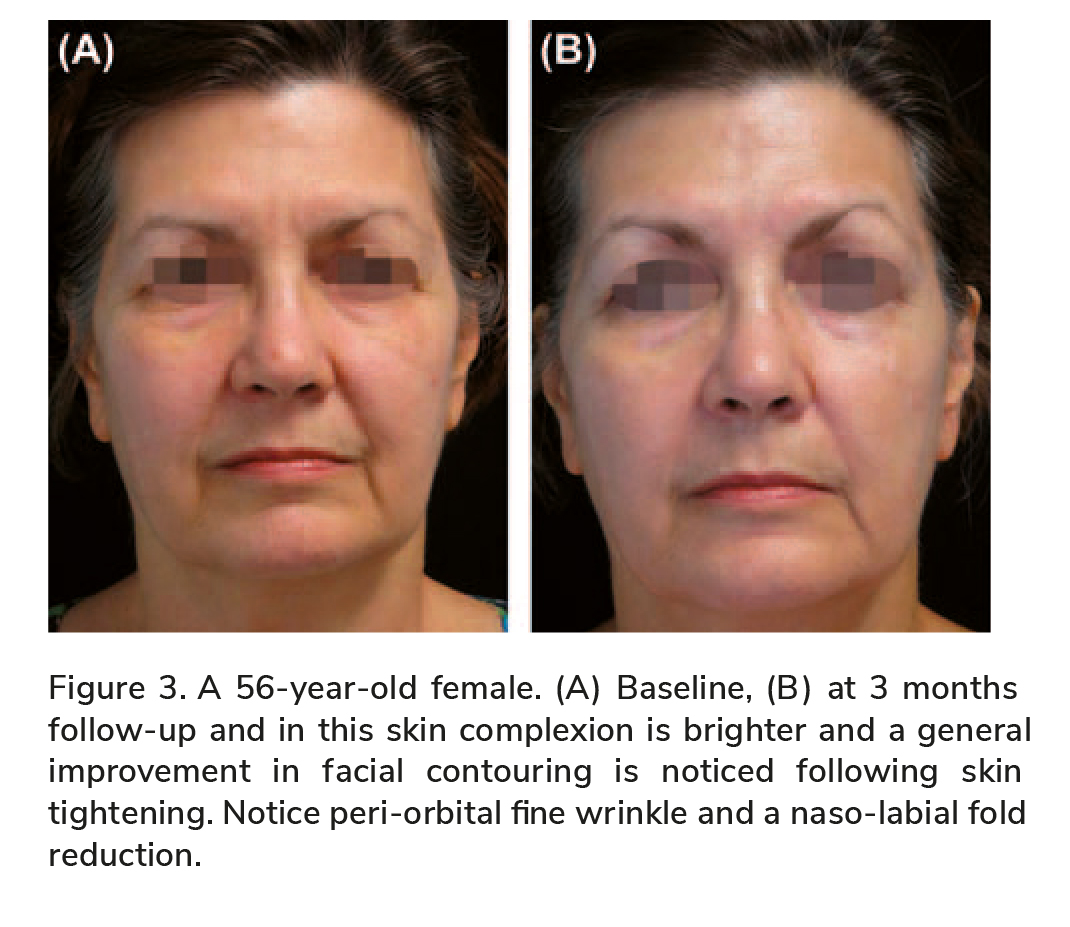
The following sets of before and after photographs
(Figures 2 – 5) illustrate the signifi cant benefi cial effect achieved by the TriFractional treatments.
In addition to the effi cacy evaluation by the two blinded evaluators, effi cacy was further demon-strated when reviewing the Fitzpatrick wrinkle and elastosis scores of the subjects as graded by each PI following a visual observation of subject ’ s skin at baseline and at 3 months follow-up visit. The average wrinkle and elastosis score given by the PIs at baseline was 4.84 (1.05) and at 3 months follow-up was 3.43 (0.97), a reduction of 1.4 (0.96) in average score.
At the 3 months follow-up visit subjects were asked to rate level of satisfaction from the treatments. Vast majority of study subjects (25 – 83.3%) noted that treatment results met their expectations to various extents, majority of study subjects (25 subjects – 83.3%) noticed an improvement of skin texture. Vast majority of study subjects (21 subjects 70%) noted that they would recommend the TriFractional treatment to friends. These results indicate that most of study subjects found the TriFractional treatment effective and tolerable.
Discussion and conclusion
Skin resurfacing and treatments of wrinkles have evolved rapidly over the past 15 years from ablative to minimally ablative methods and recently to frac-tional resurfacing.
RF skin resurfacing is an effective method for facial enhancement as the epidermis is renewed over a short time allowing for a more uniform skin tone. In the dermis, the thermal effect following epider-mal ablation results in enhanced skin tightening through re-bundling of existing collagen and through generation of new collagen via process of neocol-lagenesis that will continue several months past the procedure (16).
Hruza et al. evaluated the effect of a fractional RF applicator (Matrix ™ RF by Syneron, Israel) for skin rejuvenation and wrinkle reduction (17). Accord-ing to the authors, subjects undergoing facial treat-ments experienced minimal pain, no permanent side effects, nor signifi cant downtime. They concluded that fractional RF skin resurfacing results in a safe, tolerable and effective treatment for improvement of skin brightness, tightening, texture and for reduction of fi ne wrinkles. The depth of tissue ablation, coagu-lation, and necrosis were found to be controllable and correlated to treatment power and coverage and could be modulated to optimize treatment of variable dermatologic conditions.
In a previous publication on the A3F, clinical effects posttreatment demonstrated reduction of fi ne wrinkles, improved appearance of acne scars, a gen-eral improvement of skin texture and scar tissue, skin brightening, skin tightening, improvement of skin irregularities, and reduction in pore size (14). Histo-logical results following ex vivo and in vivo treat-ments confi rmed the pattern of fractional effect by zones of epidermal ablation with dermal collagen
condensation below accompanied with skip zones of unaffected tissue. The controlled fractional effect resulted in epidermal renewal and dermal collagen remodeling and regeneration.
In the clinical study reported in this document, treatment results demonstrated the safety and effec-tiveness of the fractional A3F for skin resurfacing allowing treatment of fi ne facial wrinkles, enhancing facial contour through skin tightening and improving complexion through epidermal renewal. As men-tioned, the immediate effect posttreatment was mostly erythema and edema followed by tiny scabs that subsided after a few days. Erythema and edema are a normal response of the infl ammatory process induced following the micro wounds created by the treatment and are an indication of an effective wound healing process (18). The micro wound healing results in a renewal of the epidermal layer and neo-collagenisis in the dermis, a process that continues several weeks after the treatment. The fractional manner of treatment with healthy intact zones allows for faster healing with no down time or discomfort to the subjects. The Principle Investigators completed
Before and After Trifractional Skin Treatment
an IRB approved questionnaire addressing their satisfaction from treatment effects, assessed skin texture improvement in 97% of the subjects (29 out of 30 subjects). A certain level of wrinkle improve-ment as a treatment outcome was mentioned for 90% of the subjects (27 out of 30 subjects).
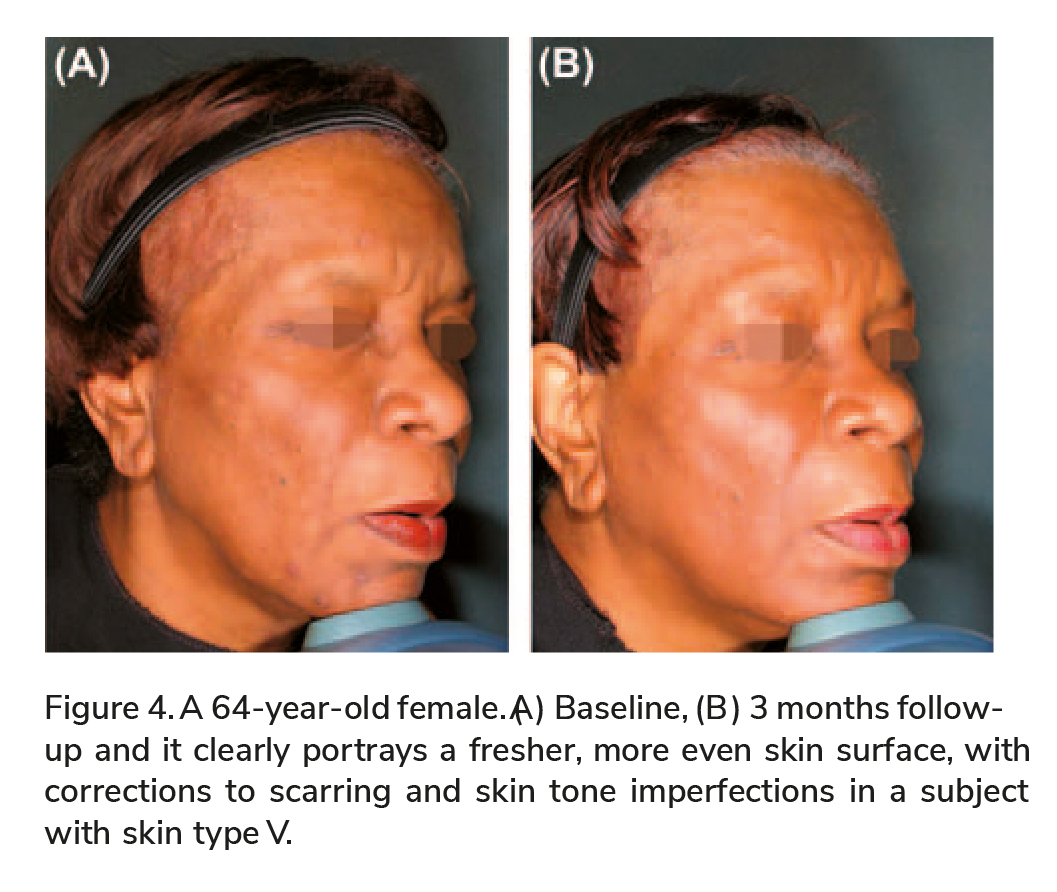
As demonstrated in Figure 4, the A3F treatment was found to be safe and effective for dark skin types resulting in improved skin complexion, evening out of skin tone and imperfections. This result indicates a major advantage of the TriFractional technology over other existing resurfacing options.

As demonstrated in Figure 4, the A3F treatment was found to be safe and effective for dark skin types resulting in improved skin complexion, evening out of skin tone and imperfections. This result indicates a major advantage of the TriFractional technology over other existing resurfacing options.
One case of posttreatment acne was reported in this study. Acne break outs have been reported as an expected side effect for patients with a history of acne following CO 2 fractional resurfacing (19).
This specifi c study was for evaluation of the A3F for treatment of wrinkles; no objective measurable data were gathered to evaluate and grade skin tone improvement, texture improvement, or general skin tightening. However, review of subjects ’ photos and subject ’ s feedback of improved skin texture defi -nitely demonstrate the effect of skin resurfacing and the evening out of skin tone imperfections, most pronounced at 1 month posttreatments, as the epi-dermal layer is freshly renewed and rejuvenated (Figure 5).
This study clearly demonstrates that the Tri Fractional technology using the A3F is a safe and effective method for skin resurfacing resulting in a reduction of wrinkles and enhanced skin and facial appearance.
Discussion and conclusion
The authors thank Julie Biron Chief Operating Offi cer, Tennessee Clinical Research Center and Enrique Echaniz, MD, Clinical Research Coordinator, Plano Site Manager, Research Across America and employees of the study site for their contribution in managing study operations.
Declaration of interest:
The authors report no confl icts of interest. The authors alone are respon-sible for the content and writing of the article. The authors thank Mira Barki, PhD for contribut-ing to the writing of this manuscript with the authors. Dr. Gold and Dr. Adelglass are consul-tants, perform research, and speak on behalf of Pollogen.
This study was funded by Pollogen Ltd.
References
1. Fisher GJ , Varani J ,Voorhees JJ. Looking older:fi broblast collapse and therapeutic implications .Arch Dermatol. 2008 ; 144 : 666 – 672 .
2. Alexiades-Armenakas MR ,Dover JS,Arndt KA . The spectrum of laser skin resurfacing: nonablative fractional and ablative laser resurfacing .J Am Acad Dermato. 2007 ; 58 : 719 – 737 .
3. Nanni CA ,Alster TS.Complications of CO 2 laser resurfacing: an evaluation of 500 patients .Dermatol Surg.1998 ; 24 : 315 – 320 .
4. Tanzi EL,Alster TS .Side effects and complications of variable pulsed erbium: YAG laser skin resurfacing: extended experience with 50 patients .Plast Reconstr Surg. 2003 ; 111 : 1524 – 1529 .
5. Manstein D ,Herron GS ,Sink RK , Tanner H ,Anderson RR .Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004 ; 3 : 426 – 438 .
6. Laubach HZ ,Tannous Z ,Anderson RR,Manstein D.Skin responses to fractional photothermolysis .Lasers Surg Med.2006 ; 38 : 142 – 149 .
7. Tierney EP ,Eisen RF ,Hanke CW. Fractional CO 2 laser skin rejuvenation.Dermatol Ther. 2011 ; 24 : 41 – 53 .
8. Chapas AM , Brightman L , Sukal S ,Hale E ,Daniel D ,Bernstein LJ ,Geronemus RG.Successful treatment of acneiform scarring with CO 2 ablative fractional resurfacing. Lasers Surg Med. 2008 ; 40 : 381 – 386 .
9. Trelles MA, V e´ lez M ,Mordon S. Correlation of histological fi ndings of single session Er:YAG skin fractional resurfacing with various passes and energies and the possible clinical implications . Lasers Surg Med.2008 ; 40 : 174 – 177 .
10. Boisnic S, Branchet MC. Ex vivo human skin evaluation of localized fat reduction and anti-aging effect by TriPollar radio frequency treatments.J Cosmet Laser Ther. 2009 early online 1 – 7 .
11. Levenberg A. Clinical experience with TriPollar radiofre-quency system for facial and body aesthetic treatments. Eur J Dermatol. 2010 ; 20 : 1 – 5 .
12. Gold MH.Tissue tightening: a hot topic utilizing deep dermal heating. J Drugs Dermatol. 2007 ; 6 : 1238 – 1242 .
13. Hantash BM ,Ubeid AA ,Chang H ,Kafi R ,Renton B.Bipolar fractional radiofrequency treatment induces neoelas-togenesis and neocollagenesis .Lasers Surg Med. 2009 ; 41 : 1 – 9 .
14. Levenberg A ,Gat A, Boisnic S ,Branchet MC. Treatment ofwrinkles and acne scars using the TriFractional, a novel frac-tional radiofrequency technology: clinical and histological results .J Cosmet Dermatol Sci App.2012 ; 2 : 117 – 125 .
15. Fitzpatrick RE ,Goldman MP ,Satur NM ,Tope WD .Pulsed carbon dioxide laser resurfacing of photo-aged facial skin .Arch Dermatol.1996 ; 132 :395 – 402 .
16. Orringer JS, Kang S , Johnson TM ,Karimipour DJ , Hamilton T ,Hammerberg C, et al .Connective tissue remodeling induced by carbon dioxide laser resurfacing of photodamaged human skin . Arch Dermatol. 2004 ; 140 : 1326 – 1332 .
17. Hruza G ,Taub AF , Collier SL, Mulholland SR.Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system . J Drugs Dermatol. 2009 ; 8 : 259 – 265 .
18. Martin P. Wound healing — aiming for perfect skin regenera-tion .Science. 1997 ; 276:75 – 86 .
19. Alster TA , Tanzi EL , Lazarus M.The use of fractional laser photothermolysis for the treatment of atrophic scars .Dermatol Surg. 2007;33:295 – 299 .









