

Clinical and histopathological results following TriPollar™
radiofrequency skin tightening treatments
Abstract
Introduction: Skin laxity, wrinkles and cellulite are common aesthetic problems associated with the aging process. These symptoms are due to the weakening and thinning of dermal connective tissue and the enlargement of hypodermal fat cells. The aim of this study was to evaluate the safety and effi cacy of the TriPollar RF technology in reducing fat and collagen regeneration. Methods: Twelve healthy patients underwent weekly treatments on different body sites using the TriPollar technology. Treatment areas were photographed and measured and patient satisfaction was monitored. One abdominal patient consented to a series of TriPollar treatments prior to her scheduled abdominoplasty. A controlled histopathology analysis was performed on skin samples taken during the abdominoplasty procedure. Results: Histopatho-logical examination revealed marked differences between treated and non-treated abdominal skin areas. An increase of 49% in dermal thickness, focal thickening of collagen fi bers and focal shrinkage of fat cells was shown following TriPollar treatments. Average patient satisfaction indicated clear satisfaction with the clinical results achieved. Conclusion: The TriPollar is a safe and effective non-invasive technology leading to skin tightening and body shaping. Histology results indicate changes at the dermal and fat layers following TriPollar treatments resulting in increased collagen regeneration and stimulated fat metabolism.
Key Words: Collagen, fat, histology, TriPollar, Omnicurrent Skin Lifting Treatment Device, RF Facial At Home, Thermal Mapping, Oxygeneo
Introduction
In recent years various non-invasive modalities have been developed for the treatment of aging skin and body contouring. One of the most popular technologies is radiofrequency (RF) treatments. RF energy is a form of electromagnetic energy. When applied to skin tissues, rapidly oscillating electromagnetic fi elds cause movement of charged particles within the tissue and the resultant electrical current generates heat proportional to the tissue electrical resistance. This source of heat has been extensively used in surgery for hemostasis and tissue ablation (electro-surgery), but more recently it has been applied as a means of shrinking redundant or lax connective tissues through the mechanism of col-lagen denaturation. Collagen molecules are produced by fi broblasts which synthesize three polypeptide chains that wrap around one another in a triple helix. The phenomenon of thermal shrinkage of collagen begins with a denaturization of the triple helix of the collagen molecule. When collagen is heated, the heat-labile intramolecular cross-links are broken and the protein undergoes a transition from a highly organized crystalline structure to a random, gel-like state (denaturation). Collagen shrinkage occurs through the cumulative effect of the ‘unwinding’ of the triple helix, due to the destruction of the heat-labile intramolecular cross-links, and the residual tension of the heat-stable intermolecular cross-links (1). Heated fi broblasts are also implicated in new collagen formation and subsequent tissue remodeling, which can also contribute to the fi nal cosmetic result. The precise heat-induced behavior of connective tissues and the extent of tissue shrink-age are dependent on several factors which include the maximum temperature reached, exposure time, tissue hydration and tissue age. Limited histological data were published on the tissue reaction to the RF energy.
RF energy can be applied to tissue between two points on the tip of a probe (bipolar) or between a single electrode tip and a grounding plate
Before and After Tripollar RF Skin Treatments

before and after tripollar rf skin treatments
(monopolar). In order to generate heat in the tissue the electrical circuit must be closed. Less current is required with a bipolar device than with a monopolar device to achieve the same effect because the current passes through a much smaller volume of tissue (2).
Initial reports to apply bipolar RF energy for collagen shrinkage were related to shoulder instability where a non-ablative RF system (CAPSure, Arthro-care Corp) was used to thermally tighten the shoul-der capsule and glenohumeral ligaments (3). Shortly following these reports, a commercial, monopolar, non-ablative RF device was introduced (ThermaCool, Thermage Inc.) for tissue tightening of facial skin (4). Using monopolar RF, this device requires an active cooling mechanism to cool the electrode that touches the skin in order to preserve the epidermis from thermal damage (5).
The regen™ (Pollogen Ltd) is a RF system that uses a multiple-electrode, TriPollar™ design. Unlike bipolar RF, the TriPollar design is based on three electrodes. One acts as a positive pole while the other two act as negative poles. The current fl owing through the common, positive pole is twice that which fl ows through each of the negative poles. To avoid over-heating of this common pole and of the tissue in contact with this pole, a sequence of electrical modulation is applied so that each electrode, in turn, acts as the common pole. Owing to this design no active cooling of the electrodes or the skin is required. The regen system delivers RF energy at a frequency of 1 MHz and a maximum power of 30 W. Two appli-cators of different sizes are available for treatment of different anatomical sites including face, neck, arms, abdomen, buttocks and thighs.
The system is indicated for the treatment of skin laxity, improvement of skin texture, treatment of cellulite and for body contouring. In this study, histological and clinical data are provided revealing the mechanism of neo-collagen production and the reduction of fat in the adipose tissue.
Materials and methods
The safety and effi cacy of the regen system for skin tightening on different body areas was evaluated by the author at the Plastic Surgery Clinic, Tel Aviv, Israel. Twelve patients between the ages of 34 and 65 years old underwent an average of seven weekly treatment sessions (a range of 4–11 treatments, protocol-customized according to individual patient needs) on different body sites, which included the face (seven), neck (four), arms (one), hands (one), and abdomen (two). Treatment areas were photographed and body areas were measured before and after treatments. One abdominal patient consented to the series of treatments prior to her scheduled abdomi-noplasty. The lower left side of her abdomen was treated while the right side was used as control. A controlled histopathology analysis was performed on skin samples taken from this patient during her

before and after tripollar neck tightening treatments
abdominoplasty procedure which was performed following seven TriPollar RF treatments.
Prior to treatment a medical history was taken to exclude any contraindication such as pregnancy, any implantable electronic device that could be disrupted by RF energy and any active dermatological or collagen-vascular disorder. Patients signed an informed consent form. Treatment areas were cleaned with soap and water, thoroughly dried and then lubricated with medical grade glycerin. Patients were provided with a ‘bio-feedback control’ which allowed them to stop the treatment in case signifi cant discomfort is felt. Facial and neck treatments were performed with the small area applicator while arms and abdominal treatments were performed with the large area applicator. Treatments were applied con-tinuously, slightly pressing and moving the applicator over the skin in a rubbing and massaging technique. A non-contact, infrared thermometer (Newtech Sources Co. Ltd) was used to monitor external skin temperature during treatment. Treatment was stopped after reaching a temperature of 40–42°C on the epidermis.
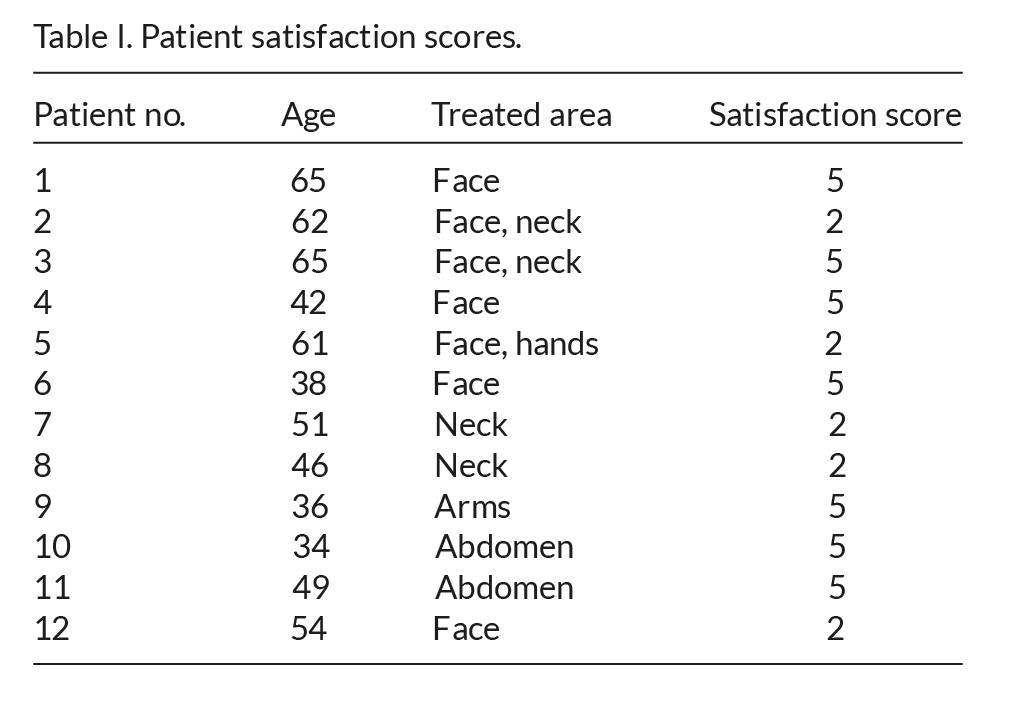
Patient satisfaction with the treatment was monitored using a fi ve-point patient assessment score (1 No satisfaction, no clinical change; 2 Low satisfaction, minor change; 3 Somewhat satisfi ed, visible change; 4 Satisfi ed, obvious change; 5 Highly satisfi ed, signifi cant change).
Three abdominal skin biopsies were taken from each of the treated and control sides: 10% formaline-fi xed, paraffi n embedded, 5-μm thick sections were prepared and stained for pathological examination by Patho-Lab Diagnostics Ltd, Ness-Ziona, Israel. The staining applied included H&E, Masson trichrome for collagen fi bers and Weigert’s elastic for elastin fi bers. Pathological examination was performed by Dr Andrea Gat, Head of Dermatopathology Unit, Sourasky Medical Center, Tel Aviv, Israel.
Results
All patients rated their satisfaction from the treat-ment outcome using a fi ve-point patient assessment score. Patient satisfaction scores are summarized in Table I.
Average patient satisfaction was 3.75, indicating clear satisfaction with achieved clinical results. Patients with thicker skin and underlying fat reported higher satisfaction with a substantial skin tightening effect, while patients with thin skin reported low satisfaction with very minimal clinical effect.
No side effects apart from transient erythema were noted.
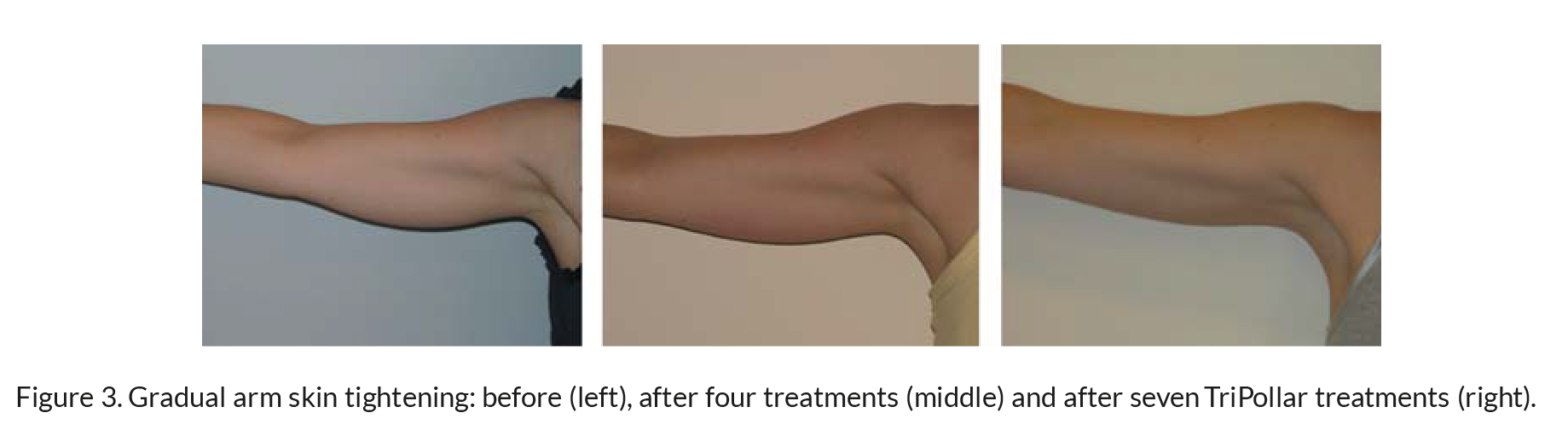
The clinical results of facial and arm skin tightening are demonstrated in Figures 1–3.
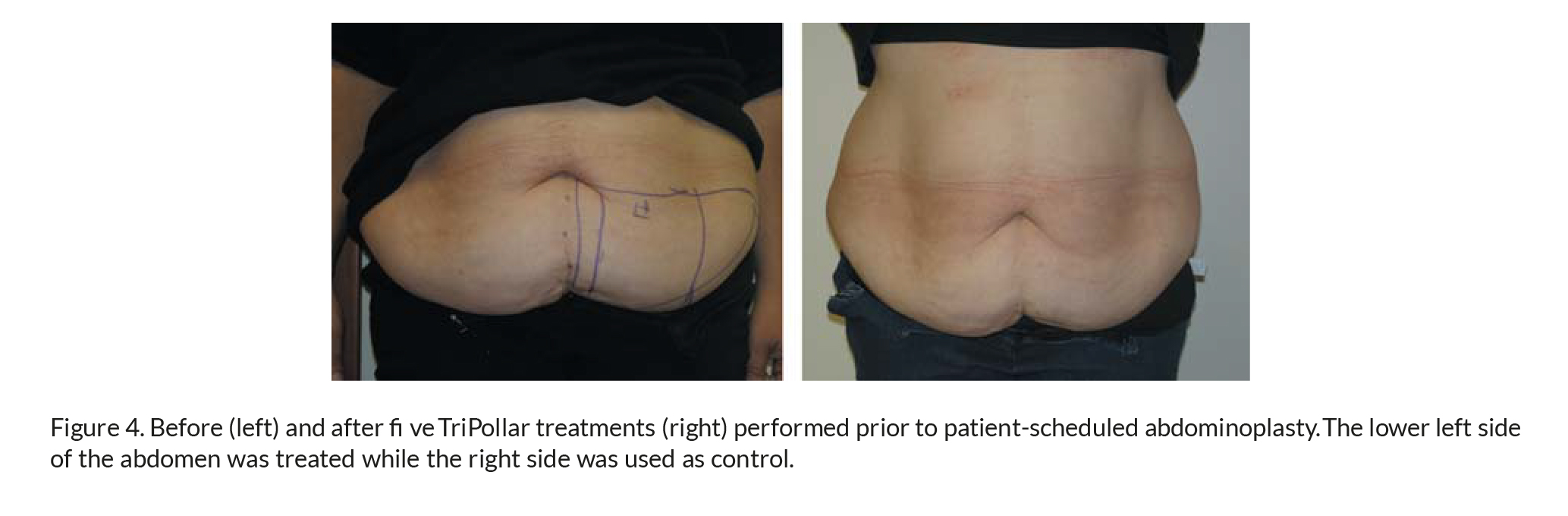
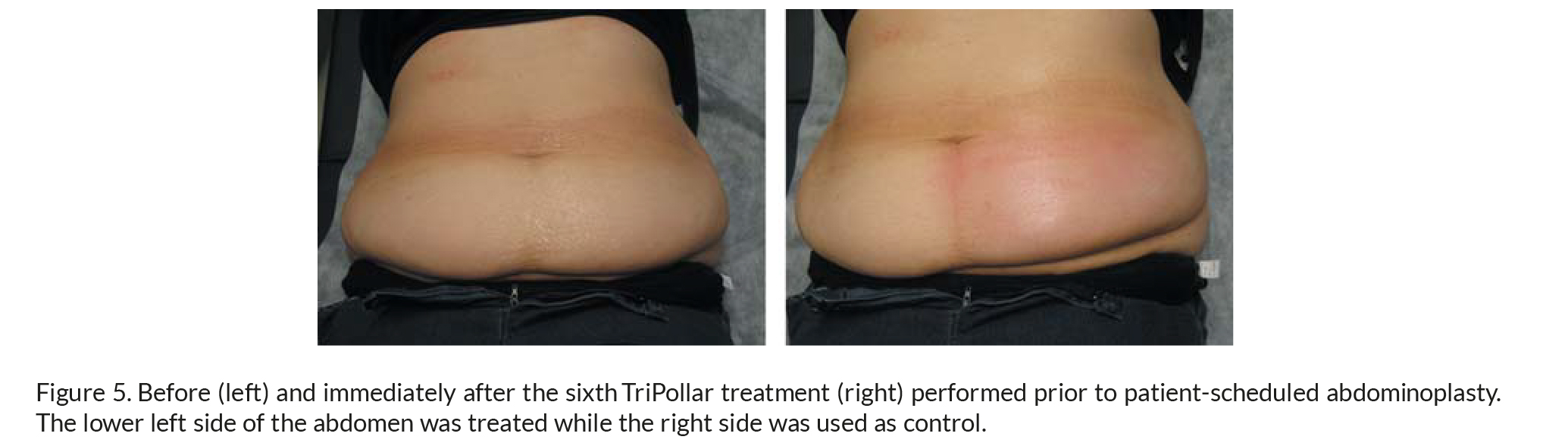
The TriPollar long-term and immediate abdominal skin tightening and fat reduction results were clinically observed by comparing the treated and untreated sides of a patient who underwent TriPollar treatments before abdominoplasty surgery (Figures 4 and 5).
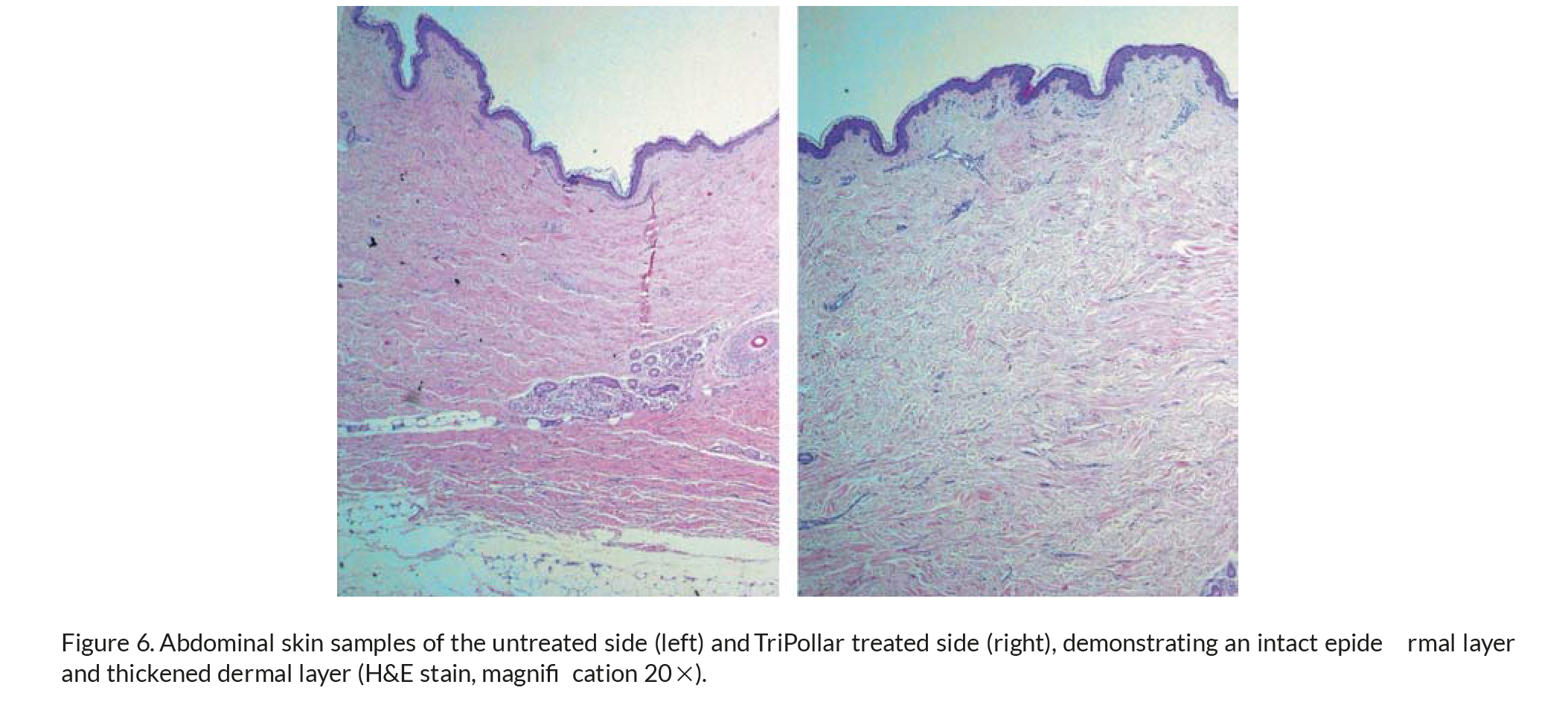
Histopathological examination of the biopsy samples revealed marked differences between the treated and non-treated abdominal skin areas. The average dermal thickness (combined papillary and
reticular layers) on the treated side was measured as 5.5 mm (range 5.0–6.0 mm), while on the non-treated side it was 3.7 mm (range 3.5–4 mm), indicating a 49% increase in dermal thickness following seven TriPollar RF treatments (Figure 6).
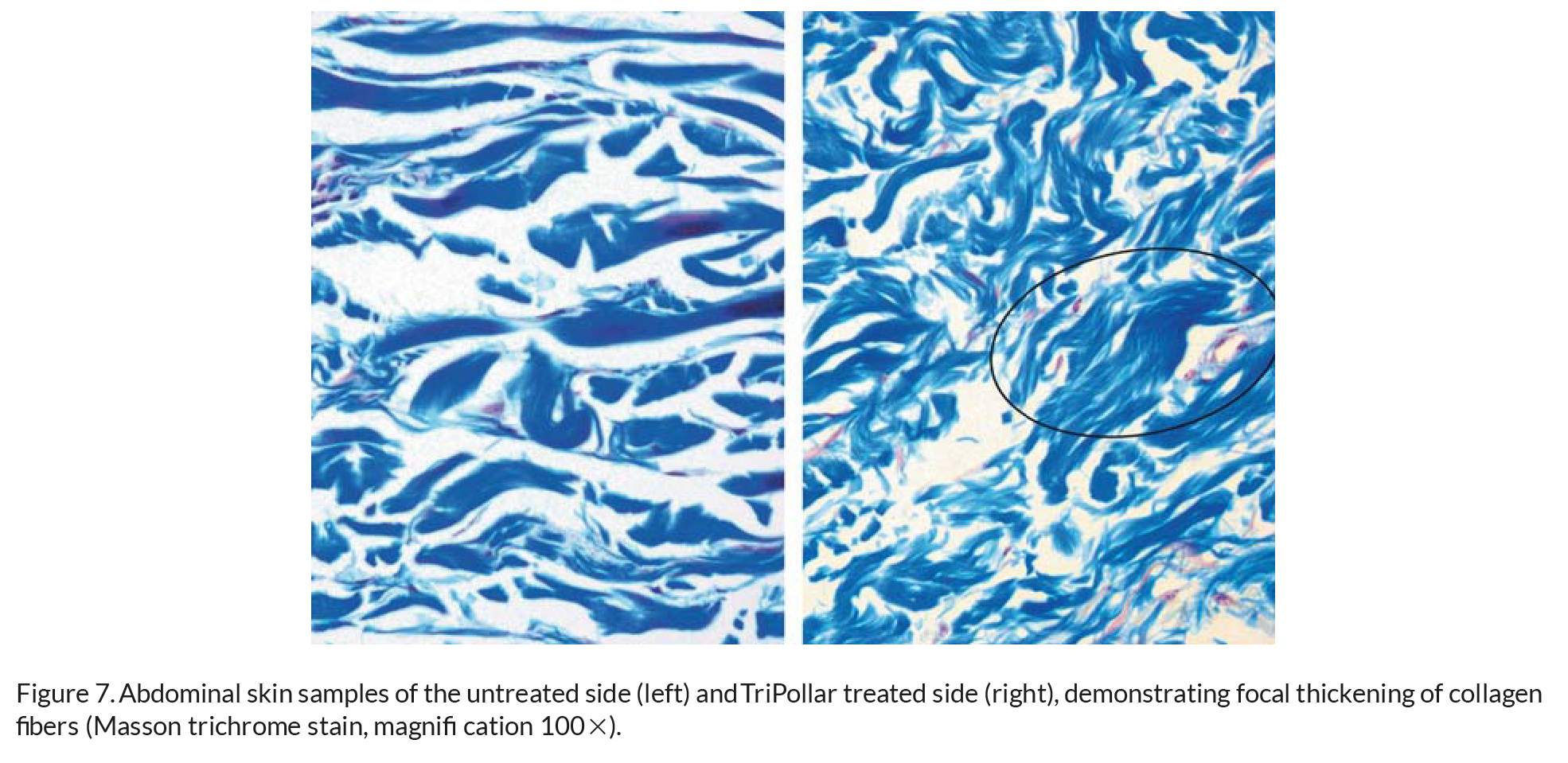
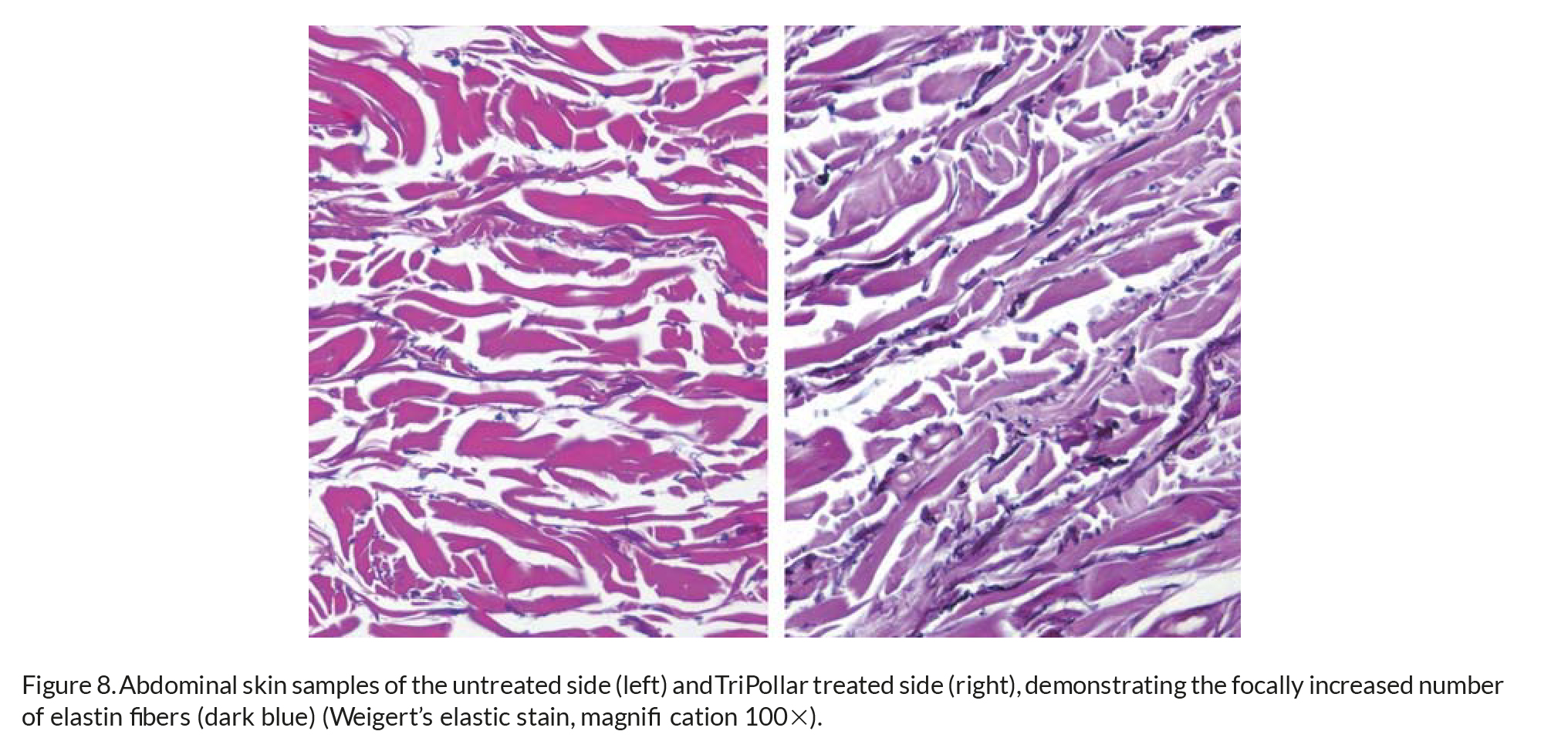
The increase in dermal thickness appears to be due to focal thickening of collagen fi bers (Figure 7). A mild increase in the number of dermal fi broblasts and focally increased number of elastin fi bers was noticed (Figure 8).
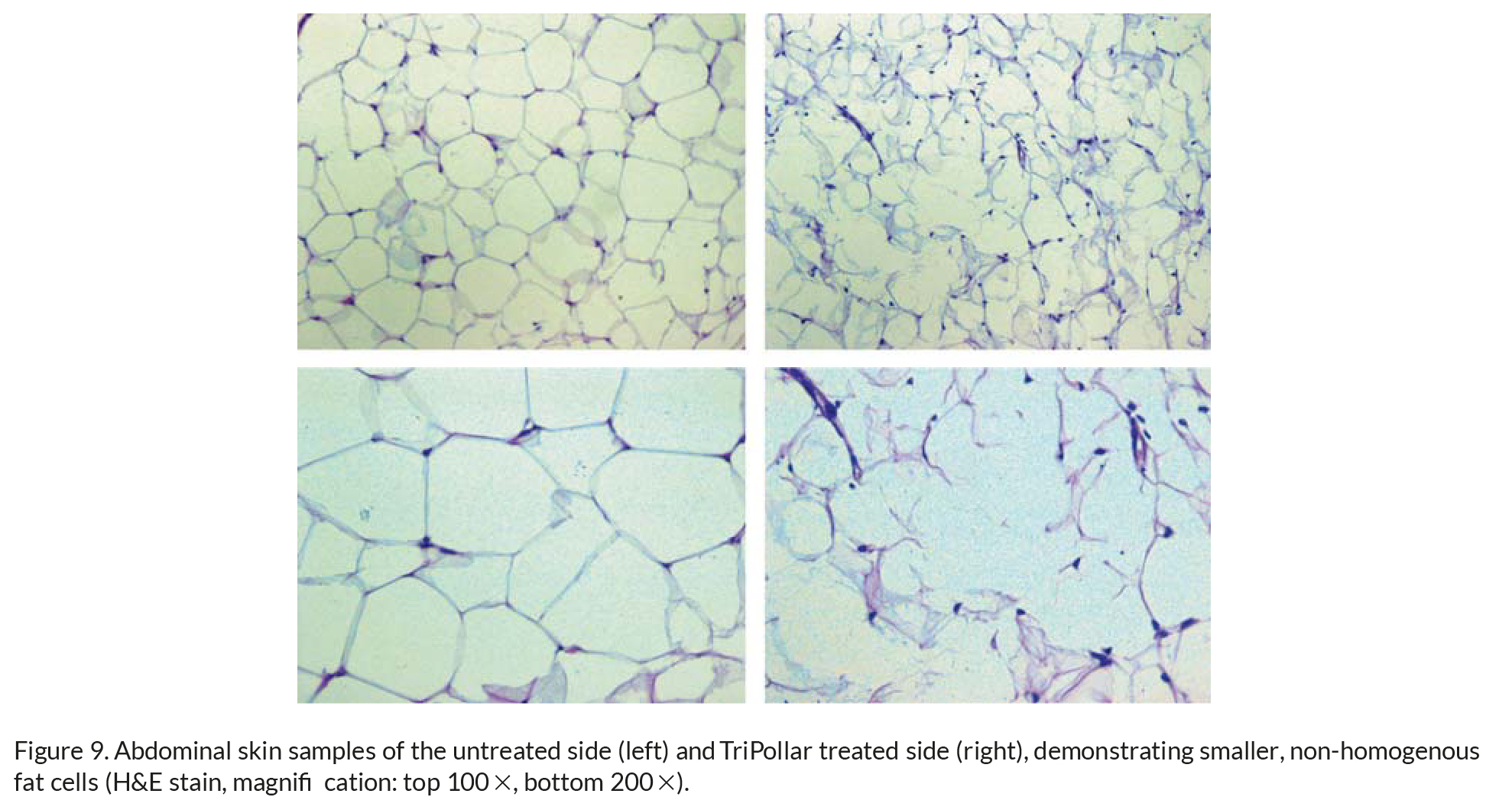
The subcutaneous layer thickness was similar in both groups; however, in some areas of the treated skin samples the lobular fat cells appear to be smaller, with elongated or polygonal irregular shapes, instead of round shapes, and with some ruptured cell membranes (Figure 9).
Infl ammatory infi ltrate or necrosis was not present in any of the samples.
Discussion
During the past decade, extensive attempts have been made to investigate the clinical and histopatho-logical effects of non-ablative energy sources on dermal structures. The fi rst such energy sources investigated for the purpose of achieving tissue tightening for wrinkle removal were the pulsed dye laser and the 1320 nm Nd:YAG laser. Alam et al. (6) published a review of histology and tissue effects following non-ablative laser and light treatments stating that though the analytic methodologies employed were limited, some generalizations can be drawn from these studies. Thermal injury most likely affects the vasculature, which initiates a cascade of infl ammatory events that includes fi broblastic proliferation and apparent up-regulation of collagen expression. Weeks to months after a series of non-ablative treatments, collagen deposition is increased and assumes a horizontal orientation parallel to the plane of the epidermis with dermal thickening reported in some of the cases.
The fi rst RF device aimed at skin tightening was initially studied using a standard guinea pig model (7). With this monopolar device, dermal heating as shallow as the papillary dermis or as deep as the subcutaneous fat was achieved. The results showed that heating the dermal layer of the skin is associated with collagen denaturation and subse-quent thickening and shortening of collagen fi brils. This is followed by a period of increased fi broblast activity and neo-collagen formation over a period of several months. Histological changes associated with new collagen formation in the dermis were noted in the treatment areas where signifi cant skin contraction was observed.
Emilia del Pino et al. (8) reported on the effect of monopolar RF on cellulite and subcutaneous tissue of the buttocks and thighs. They administered two RF treatments spaced 15 days apart on 26 healthy female patients with visible bilateral cellulite on either the buttocks or the thighs. RF volumetric tissue heating was delivered in three passes of 30 seconds each. Results were analyzed using real-time ultrasound imaging. From the measurements of
the distance between the stratum corneum to the Camper’s fascia and from the stratum corneum to the muscle they were able to demonstrate that 68% of the patients presented a contraction of the volume of approximately 20%. When analyzing the changes in the Camper’s fascia between the fi rst session and 45 days later, they repeatedly observed a noticeable organization of the fi brous lines, as well as an increase of the fi brous tissues in 53% of the cases, and an increase of the thickness of the fi bers in 57% of the cases. Most patients were satisfi ed with the results; the most satisfi ed were the women who had had the most accentuated defects.
Goldberg et al. (9) reported clinical, histological and MRI analysis of cellulite treatment with a uni-polar RF device. This device allows heat penetration into tissue to a depth of 15–20 mm. A total of 30 subjects with upper thigh cellulite were treated every other week for a total of six treatments. Epidermal skin temperature of 40–42ºC was maintained during treatment. Twenty-seven subjects showed evidence of clinical improvement with a mean decrease in leg circumference of 2.45 cm. Histologies demonstrated dermal fi brous band thickening. Unlike del Pino’s fi ndings, no changes in the pannicular layer, including Camper’s fascia, were noted at the 6-month follow-up. They thus hypothesized that while RF may initially promote deep tightening, it is, at the end of 6 months, dermal fi brosis that leads to the longer-lasting results. Montesi et al. (10) reported clinical and histo-logical results using a bipolar RF device accompanied by vacuum-assisted positioning and folding of the skin for the treatment of wrinkles, skin laxity, acne scars and striae distensae. Thirty patients underwent a cycle of six to eight sessions with 2-week intervals.
RF treatment was applied not only to the desired treated areas, such as the periorbital region, but also to distal areas such as forehead and temple regions, in order to improve the overall collagen contraction effect. Results were monitored photographically. In addition, 15 patients were subjected to two biopsies, one at the start of treatment and the other 3 months following the last treatment. All patients showed improvement in treated imperfections from the second session onwards and expressed satisfaction at the end of the treatment cycle. The most notable results were observed in striae distensae. Temporary side effects consisted of rashes and ecchymosis. In two cases, blisters were caused by excessive RF set-tings. Indeed, 3-mm punch biopsies confi rmed the clinical results observed. Biopsies of untreated skin showed atrophic and intensely elastotic dermal col-lagen while treated skin showed a decrease in colla-gen atrophy as well as an increase in interstitial edema indicative of better dermal trophism. Patients over 60 years old or with a high degree of photodamage showed less signifi cant clinical and histological improvement than younger or less photodamaged patients. In biopsies performed on the striae, a marked decrease in sclerosis together with an increase in the organization of collagen fi bers was observed. Preliminary clinical and histological results obtained with the regen TriPollar RF system appear to be in line with those previously reported for both monopolar and bipolar RF systems. Collagen shrink-age and thickening appear to be responsible for the short-term skin tightening effect and longer-lasting
84 H. Kaplan & A. Gat
remodeling effects as previously reported. Fat cell shrinkage seems to be due to accelerated natural fat metabolism by the release of free fatty acids from the fat cells. The correlation between the extent of clinical effect and skin thickness is further investigated. The TriPollar system does not require skin cooling, obtains measureable results and has high patient satisfaction without the need for any auxiliary treatment modal-ities. The treatment is extremely safe and easy to apply. The availability of applicators with various sizes optimizes the treatment of different anatomical sites such as the face, neck, arms, abdomen and thighs.
Summary
The regen TriPollar device is a high-power, multipo-lar, RF system that can safely and effectively be used for body contouring, particularly on the abdomen, thighs and arms, as well as for the treatment of cel-lulite, skin laxity and facial wrinkles. Application of this treatment modality is simple, non-invasive and extremely safe on all skin types. Clinical and histo-logical results have been documented and appear to be maintained for at least several months following a typical treatment course of 8 weekly sessions.
Declaration of interest: The authors report no confl icts of interest. The authors alone are responsible for the content and writing of the paper.
References
1. Arnoczky SP, Aksan A. Thermal modifi cation of connective tissues: basic science considerations and clinical implications. J Am Acad Orthop Surg. 2000;8:305–13.
2. Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. Lasers Surg Med. 2004;34:91–7.
3. Lopez MJ, Hayashi K, Fanton GS, Thabit G 3rd,Markel MD. The effect of radiofrequency energy on the ultra-structure of joint capsular collagen. Arthroscopy. 1998;14:495–501.
4. Ross EV, et al. A new non-ablative radiofrequency technology for skin tightening application. American Academy of Dermatology Annual Meeting, 2000.
5. Hsu TS, Kaminer MS. The use of nonablative radiofrequency technology to tighten the lower face and neck. Semin Cutan Med Surg. 2003;22:115–23.
6. Alam M, Hsu TS, Dover JS, Wrone DA, Arndt KA.Nonablative laser and light treatments: histology and tissue effects – A review. Lasers Surg Med. 2003;33:30–9.
7. Hardaway CA, Ross EV. Nonablative laser skin remodeling.Dermatol Clin. 2002;20:97–111.
8. Emilia del Pino M, Rosado RH, Azuela A, Graciela Guzman M, Arguelles D, Rodriguez C, et al. Effect of controlled volumetric tissue heating with radiofrequency on cellulite and the subcutaneous tissue of the buttocks and thighs. J Drugs Dermatol. 2006;5:714–22.
9. Goldberg DJ, Fazeli A, Berlin AL. Clinical, laboratory, and MRI analysis of cellulite treatment with a unipolar radiofre-quency device. Dermatol Surg. 2008;34:204–9; discussion 209. Epub 2007 Dec. 17.
10. Montesi G, Calvieri S, Balzani A, Gold MH. Bipolar radio-frequency in the treatment of dermatologic imperfections: clinicopathological and immunohistochemical aspects. J Drugs Dermatol. 2007;6:890–6.








